
Respiratory and Airway Management — MCQs

On this page
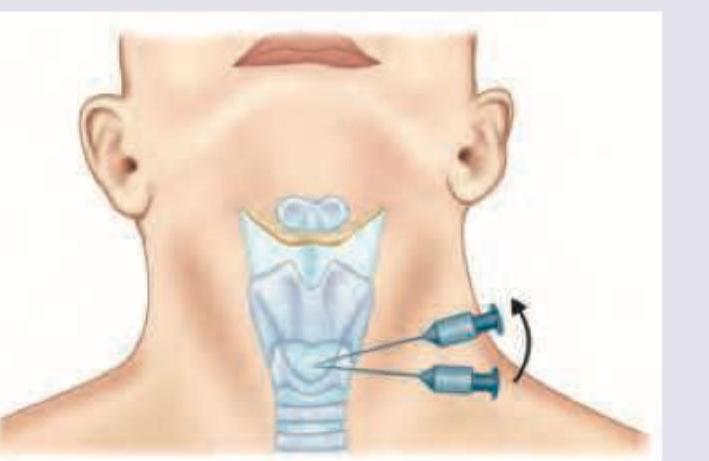
All are correct about the procedure being performed except: (Recent NEET Pattern 2016-17)
Which is correct about the laryngoscope blades shown below? (Recent NEET Pattern 2016-17)

Which is correct about the instrument shown?

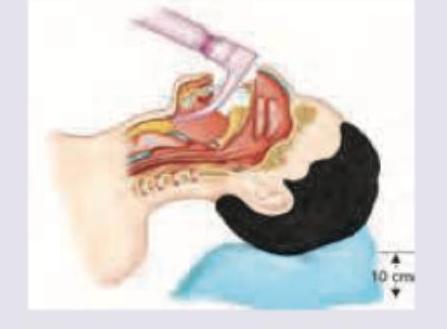
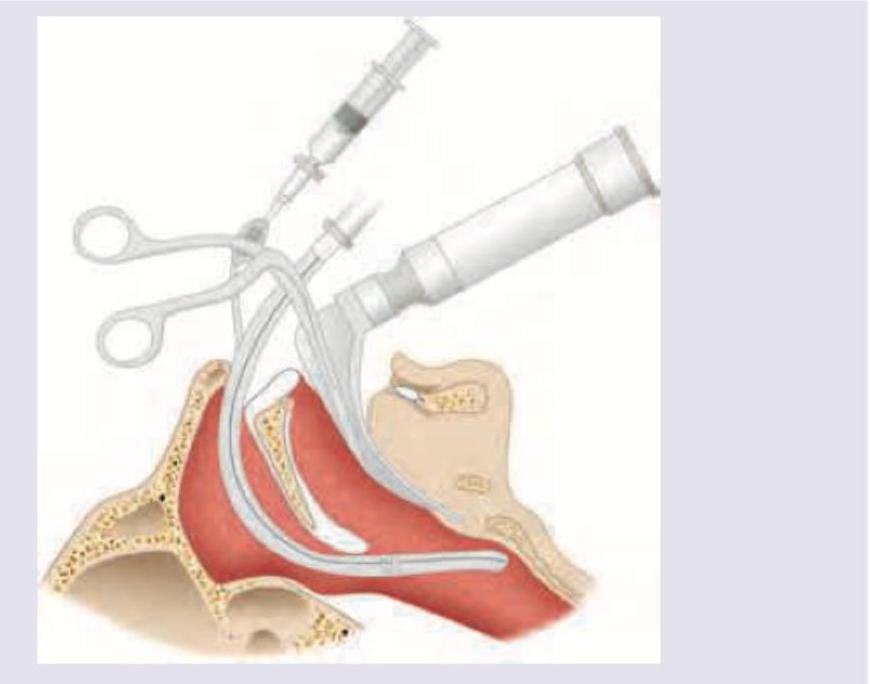
A construction worker met with an accident when a cement block fell on his face. He sustained severe maxillofacial and laryngeal injury. He was not able to open his mouth and is having jaw fracture with obstruction in nasopharynx and oropharynx. To stabilize his airway, the following procedure was done on him. Which option describes the procedure done on him?
The equipment shown below is used for:

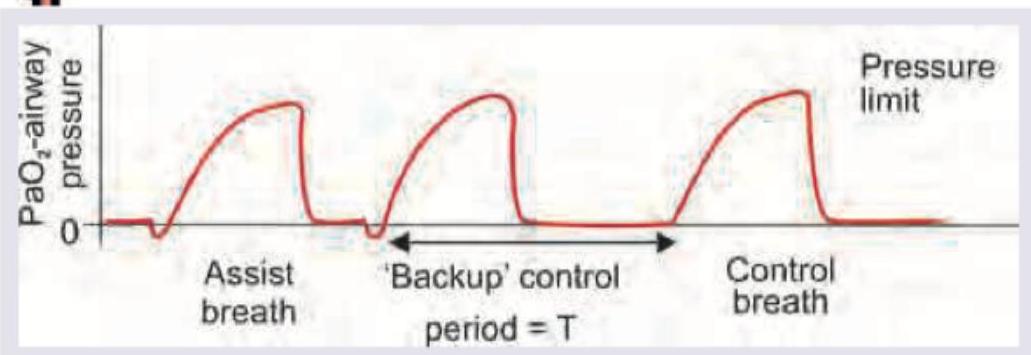
What is the mode of ventilation shown here?

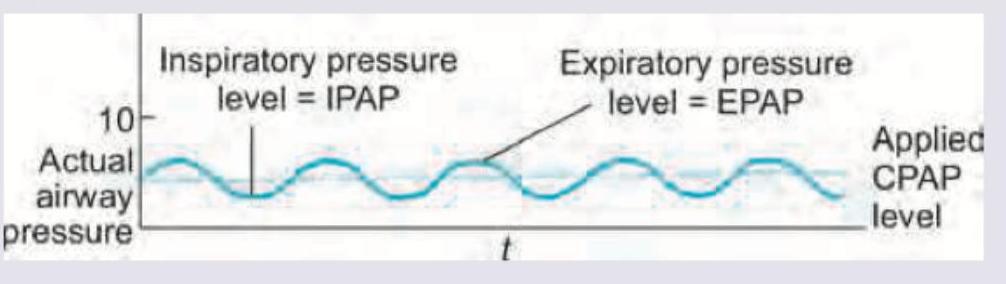
What is the mode of ventilation shown here?
The following ventilation modality is used in:
(1) Name the forceps being used in the procedure being performed:
Maximum oxygen concentration can be delivered by:
Practice by Chapter
Respiratory Physiology
Practice Questions
Airway Anatomy
Practice Questions
Preoxygenation Techniques
Practice Questions
Mask Ventilation
Practice Questions
Supraglottic Airway Devices
Practice Questions
Direct Laryngoscopy
Practice Questions
Video Laryngoscopy
Practice Questions
Fiberoptic Intubation
Practice Questions
Surgical Airway Management
Practice Questions
One-Lung Ventilation Techniques
Practice Questions
Ventilation Strategies During Anesthesia
Practice Questions
Extubation Criteria and Techniques
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app