
Respiratory and Airway Management — MCQs

On this page
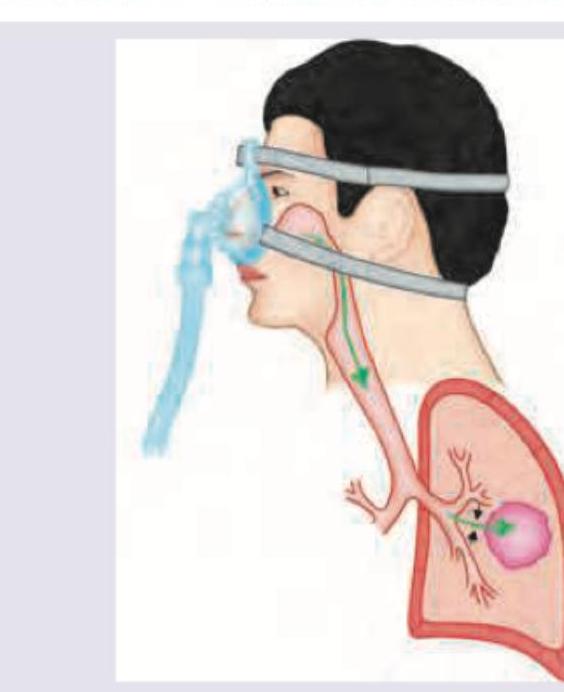
The mode of ventilation shown below is used for:
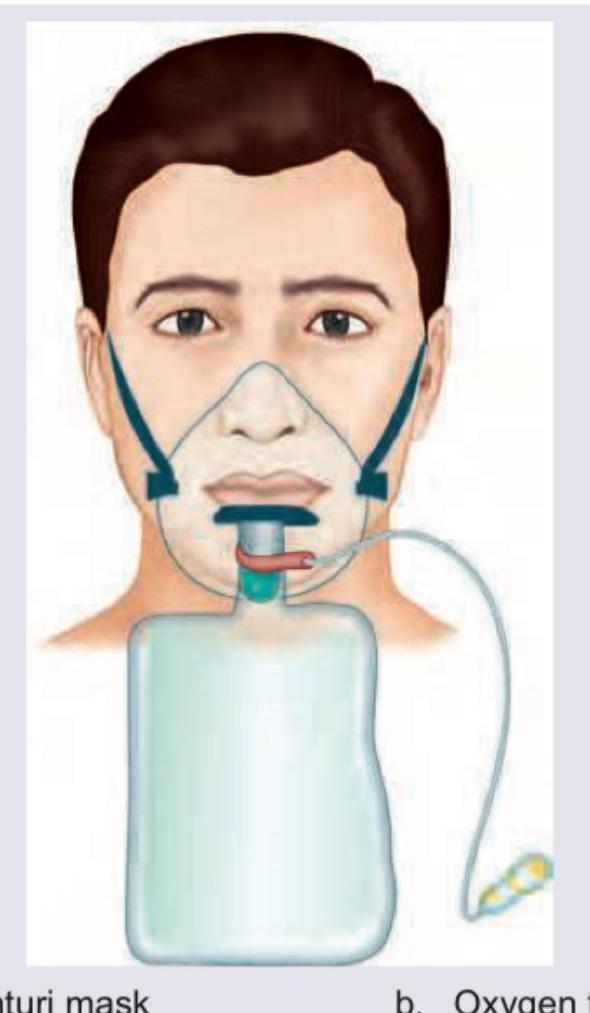
The following image shows:
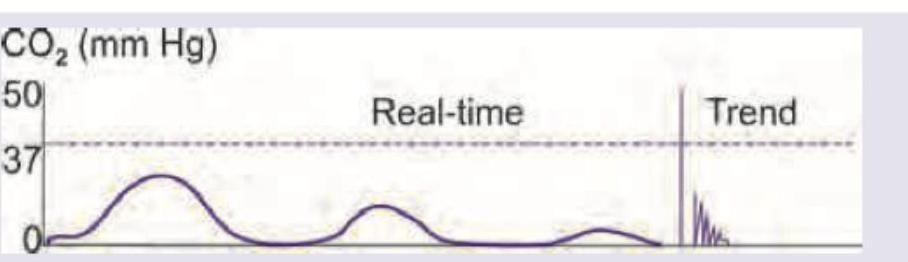
A patient is scheduled for emergency laparotomy for a perforated duodenal ulcer. He was administered 2 L of fluid and was wheeled into the OT. He was intubated and capnography recording shows the following recording. This indicates:
All are correct about airway management shown below except:

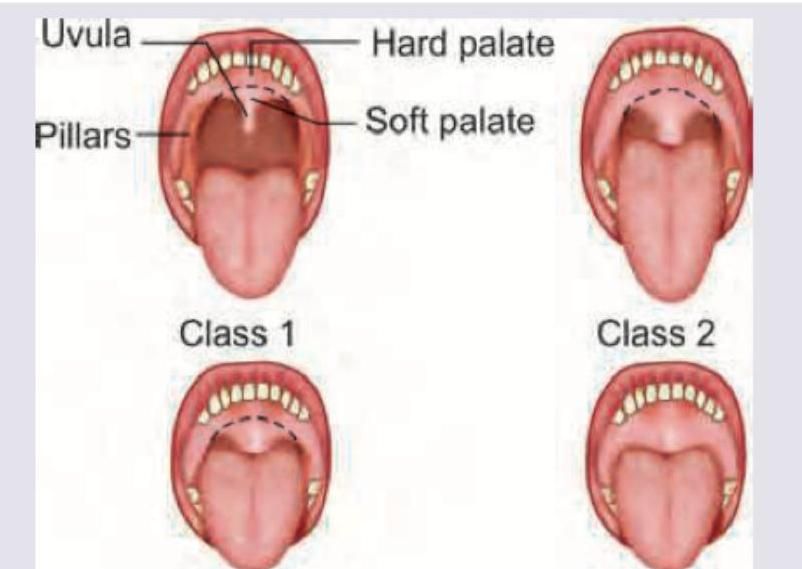
What is the grade of laryngeal view?
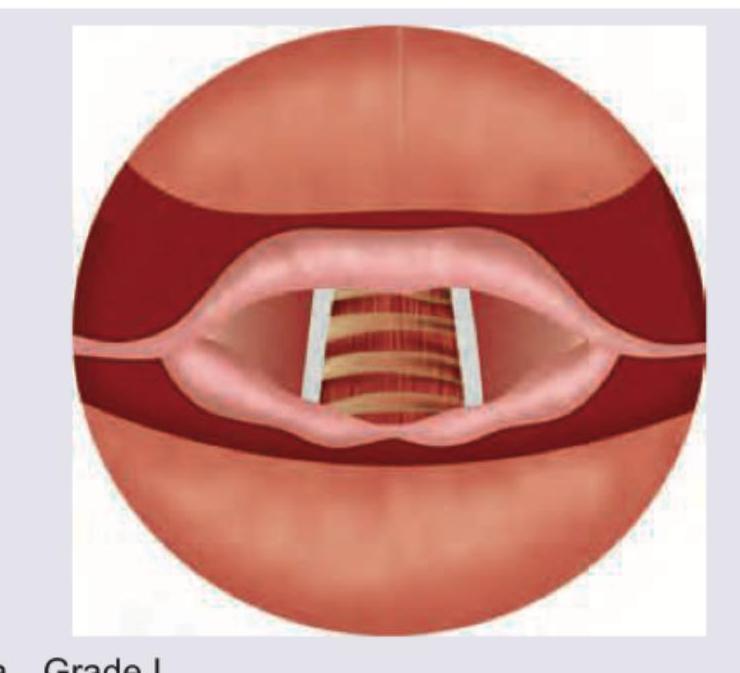
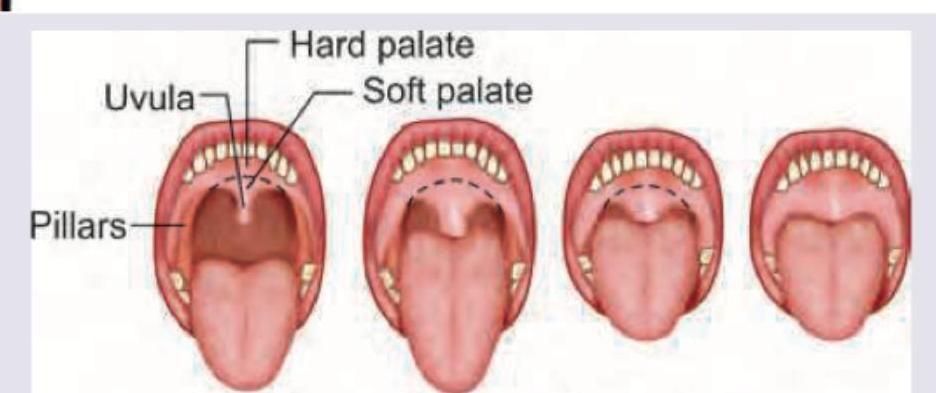
What is this classification used for?
All are correct about the image shown except:
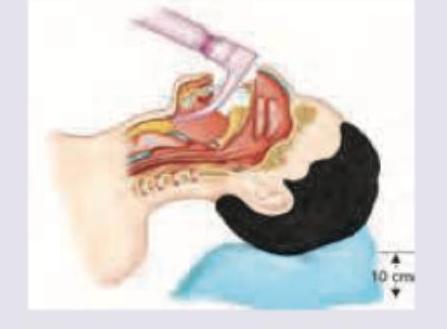
In correct positioning the tip of the instrument shown in the image should lie at:
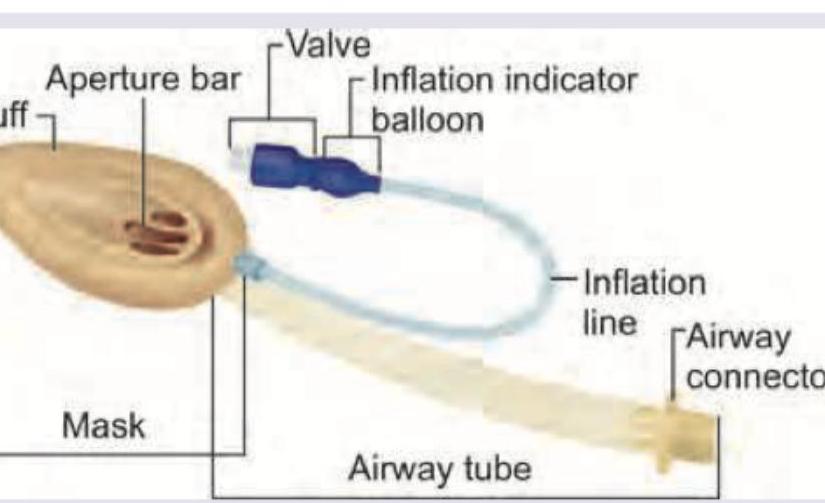
All are correct about the airway device shown below except: (Recent NEET Pattern 2016-17)

All are correct about the procedure being performed except: (Recent NEET Pattern 2016-17)
Practice by Chapter
Respiratory Physiology
Practice Questions
Airway Anatomy
Practice Questions
Preoxygenation Techniques
Practice Questions
Mask Ventilation
Practice Questions
Supraglottic Airway Devices
Practice Questions
Direct Laryngoscopy
Practice Questions
Video Laryngoscopy
Practice Questions
Fiberoptic Intubation
Practice Questions
Surgical Airway Management
Practice Questions
One-Lung Ventilation Techniques
Practice Questions
Ventilation Strategies During Anesthesia
Practice Questions
Extubation Criteria and Techniques
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app