
Respiratory and Airway Management — MCQs

On this page
An infant with respiratory distress was intubated. What is the fastest and most accurate method to confirm endotracheal tube placement?
Which is the anesthetic agent of choice in a case of status asthmaticus?
What is the maximum fraction of inspired oxygen (FiO2) that can be delivered via a nasal oxygen catheter?
A patient under anesthesia is found to be in a “cannot intubate, cannot ventilate” (CICV) scenario. What is the next best step in management?
What is the primary function of the inflatable cuff of the endotracheal tube shown in the image?

A patient undergoing general anesthesia develops left lung collapse following intubation. On auscultation, breath sounds are heard only on the right side. What is the most likely cause of this condition?
Which of the following is the use of the Mallampatti classification?
A patient in the ICU with an endotracheal tube now needs a tracheostomy tube. Which type of tube will you use?
Which of the following airway devices helps maintain Fio2 of 0.25-0.60, irrespective of the patient's breathing effort?
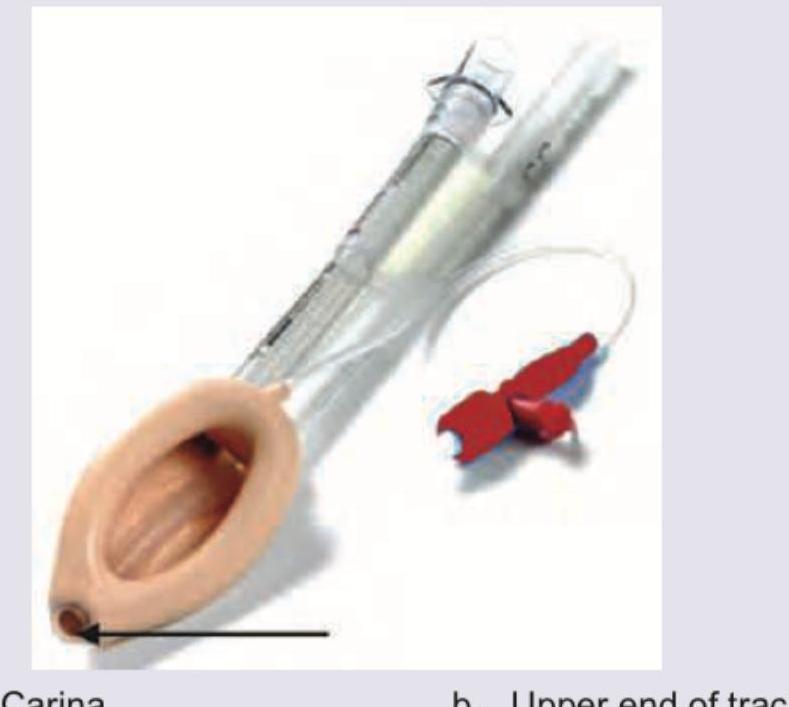
The diagram of a correctly positioned proseal-type Laryngeal Mask Airway is provided below. Above what site is the arrow marked area of the airway positioned?
Practice by Chapter
Respiratory Physiology
Practice Questions
Airway Anatomy
Practice Questions
Preoxygenation Techniques
Practice Questions
Mask Ventilation
Practice Questions
Supraglottic Airway Devices
Practice Questions
Direct Laryngoscopy
Practice Questions
Video Laryngoscopy
Practice Questions
Fiberoptic Intubation
Practice Questions
Surgical Airway Management
Practice Questions
One-Lung Ventilation Techniques
Practice Questions
Ventilation Strategies During Anesthesia
Practice Questions
Extubation Criteria and Techniques
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app