
Respiratory and Airway Management — MCQs

On this page
Blind nasal intubation is indicated in which of the following conditions?
Which muscle relaxant can be used as an alternative to succinylcholine for endotracheal intubation?
By which hand should a right-handed person hold the laryngoscope for intubation?
Difficult oral intubation may be associated with all EXCEPT:
What is the reason for difficult intubation in an obese patient?
What is the standard airway intervention for Ludwig's Angina?
What difficulty is assessed by the Mallampati classification during intubation?
What is the role of the Mallampati classification in preanesthetic evaluation?
In tracheotomy, what is the typical reduction in dead space?
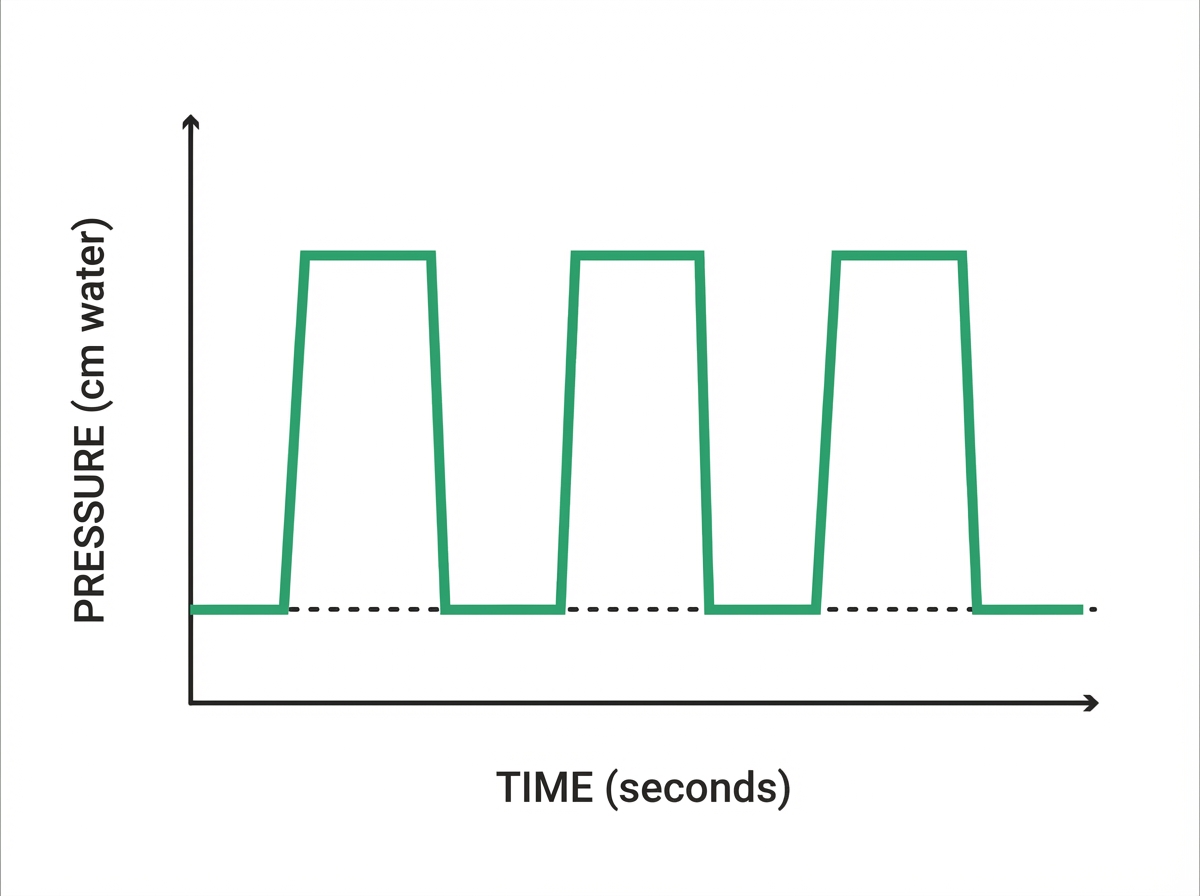
What mode of ventilation is characterized by the pressure-time graph shown, which demonstrates time-cycled mandatory breaths at a fixed inspiratory time?
Practice by Chapter
Respiratory Physiology
Practice Questions
Airway Anatomy
Practice Questions
Preoxygenation Techniques
Practice Questions
Mask Ventilation
Practice Questions
Supraglottic Airway Devices
Practice Questions
Direct Laryngoscopy
Practice Questions
Video Laryngoscopy
Practice Questions
Fiberoptic Intubation
Practice Questions
Surgical Airway Management
Practice Questions
One-Lung Ventilation Techniques
Practice Questions
Ventilation Strategies During Anesthesia
Practice Questions
Extubation Criteria and Techniques
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app