
Local Anesthetics — MCQs

On this page
Which of the following procedures is NOT an appropriate indication for the use of this cream?
What type of local anesthesia involves injecting the anesthetic directly into the tissue at the site of the procedure?
Which of the following local anesthetics is not used topically?
Which of the following statements about lidocaine is FALSE?
Which of the following local anesthetics has the longest duration of action?
What is the concentration of adrenaline used with lidocaine?
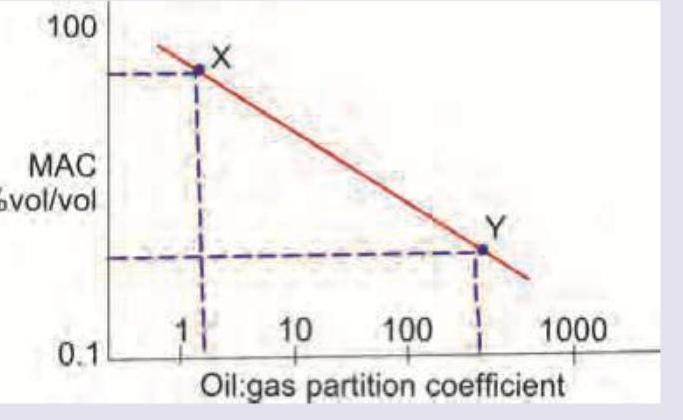
Which is correct about the anesthetic drugs X and Y in the image shown? (Recent NEET Pattern 2016-17)
The composition of the given anesthetic product is:
A young male was administered regional anesthesia with 0.25% bupivacaine. The patient became unresponsive, and the pulse became unrecordable. What is the best management in this situation?
Which nerve is targeted in the nasociliary nerve block?
Practice by Chapter
Chemistry and Mechanism of Action
Practice Questions
Pharmacokinetics of Local Anesthetics
Practice Questions
Amide Local Anesthetics
Practice Questions
Ester Local Anesthetics
Practice Questions
Clinical Uses of Local Anesthetics
Practice Questions
Toxicity of Local Anesthetics
Practice Questions
Management of Local Anesthetic Systemic Toxicity
Practice Questions
Adjuvants to Local Anesthetics
Practice Questions
Maximum Safe Doses
Practice Questions
Local Anesthetics in Special Populations
Practice Questions
Allergic Reactions to Local Anesthetics
Practice Questions
Future Developments in Local Anesthetics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app