
Complications in Anesthesia — MCQs

On this page
All are true statements about malignant hyperthermia except?
Which of the following is true regarding post-spinal headache?
In which patient position is venous air embolism most commonly encountered?
A patient under inhalational anesthesia suddenly develops fever, increased heart rate and BP, acidosis, and arrhythmia during surgery. What is your first step of intervention?
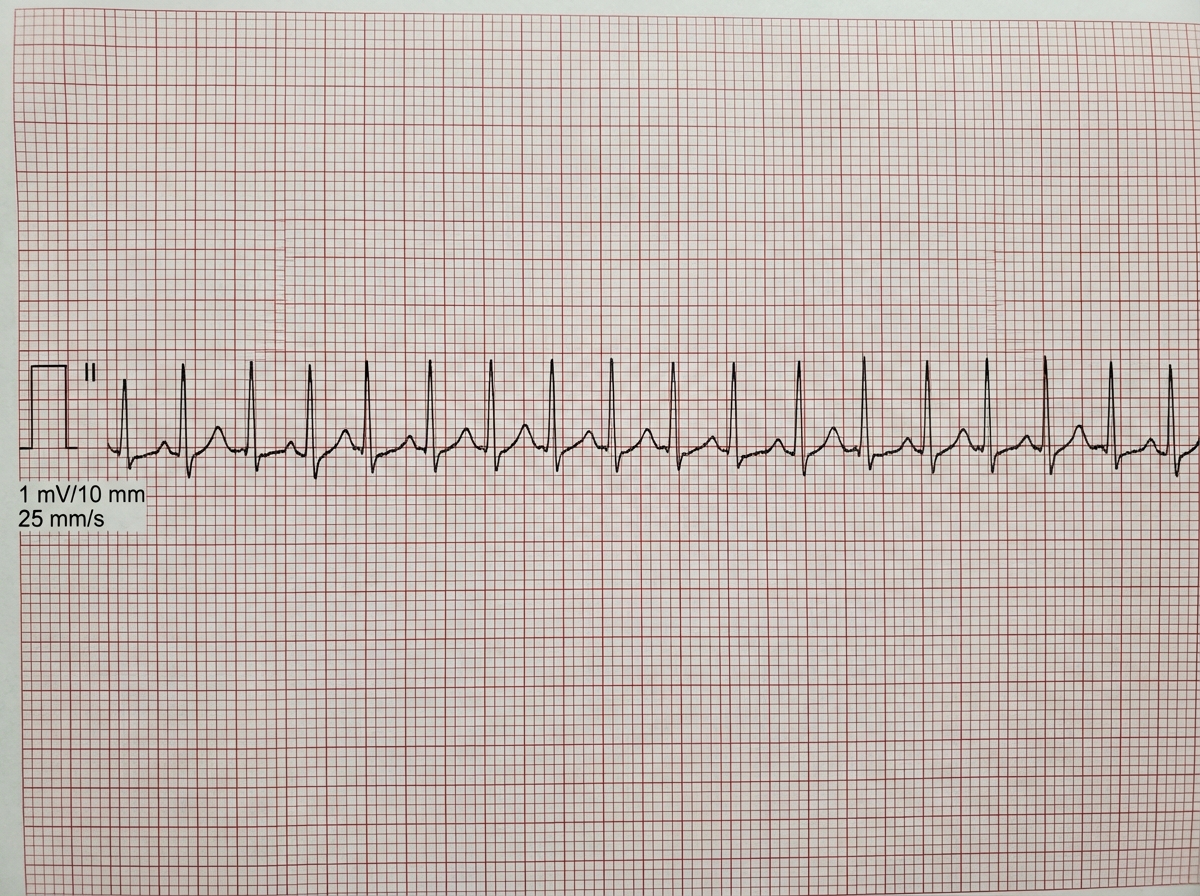
A hemodynamically stable patient develops sinus tachycardia as shown in the ECG below, intra-operatively. Reversible causes such as inadequate anesthesia, hypovolemia, hypoxia, hypercarbia, and pain have been excluded or corrected. What is the drug of choice (DOC)?
Which of the following is NOT a complication of surgery performed in the sitting position?
A severely ill patient was maintained on an infusional anesthetic agent. On the 2nd day, he started deteriorating. What is the probable culprit?
In all of the following conditions, hyperkalemia produced by succinylcholine is exaggerated, except?
Which of the following anesthetic agents is known to be hepatotoxic?
What is the most common cause of death after anesthesia?
Practice by Chapter
Adverse Drug Reactions
Practice Questions
Anaphylaxis and Allergic Reactions
Practice Questions
Malignant Hyperthermia
Practice Questions
Local Anesthetic Toxicity
Practice Questions
Perioperative Cardiac Complications
Practice Questions
Pulmonary Complications
Practice Questions
Awareness Under General Anesthesia
Practice Questions
Neurological Complications
Practice Questions
Postoperative Visual Loss
Practice Questions
Perioperative Renal Dysfunction
Practice Questions
Transfusion-Related Complications
Practice Questions
Risk Management and Prevention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app