
Complications in Anesthesia — MCQs

On this page
A known case of hyperthyroidism, who is not on medication, is scheduled for total thyroidectomy. The PAC check was not done properly. What is the leading complication that can occur during surgery?
A patient undergoing surgery is administered succinylcholine for muscle relaxation. Shortly after administration, he develops hyperthermia, muscle rigidity, tremors, and tachycardia. What is the most appropriate treatment for this condition?
A 35-year-old male undergoing abdominal surgery under general anesthesia develops sudden generalized muscle rigidity, rapid increase in body temperature, and tachycardia shortly after administration of sevoflurane and succinylcholine. His end-tidal CO2 is rising despite controlled ventilation. What is the most appropriate immediate treatment?
A patient undergoing surgery receives a muscle relaxant and soon develops flushing and rashes over the neck and anterior chest. Which of the following muscle relaxants is most commonly associated with this reaction?
All are correct about the complications of the anesthesia technique shown except:

All of the following reduce complication rates following the procedure shown below, except:

During induction of anesthesia, after thiopentone injection patient develops discoloration of hand. All are true about this condition and its management except:

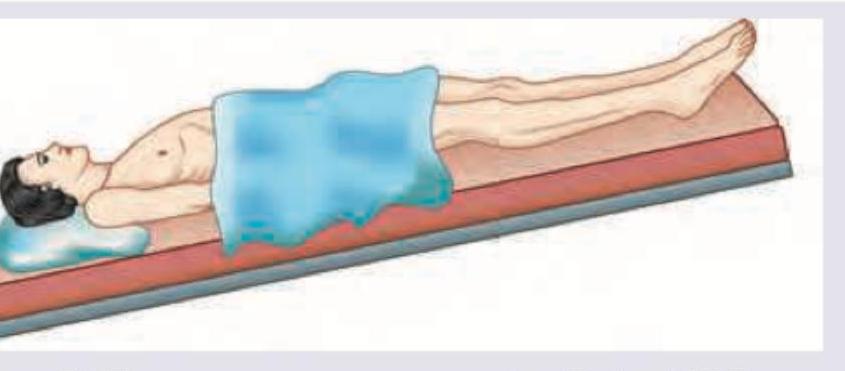
The position of the patient as shown below is favored for which of the following conditions?
Which one of the following is a Nephrotoxic anaesthetic agent ?
In which clinical scenario would you find a patient requiring the vital signs assessment technique shown in the image?

Practice by Chapter
Adverse Drug Reactions
Practice Questions
Anaphylaxis and Allergic Reactions
Practice Questions
Malignant Hyperthermia
Practice Questions
Local Anesthetic Toxicity
Practice Questions
Perioperative Cardiac Complications
Practice Questions
Pulmonary Complications
Practice Questions
Awareness Under General Anesthesia
Practice Questions
Neurological Complications
Practice Questions
Postoperative Visual Loss
Practice Questions
Perioperative Renal Dysfunction
Practice Questions
Transfusion-Related Complications
Practice Questions
Risk Management and Prevention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app