
Cardiovascular Anesthesia — MCQs

On this page
What is true regarding cardiopulmonary resuscitation?
During surgery for aortic arch aneurysm under deep hypothermic circulatory arrest, which of the following anesthetic agents administered prior to circulatory arrest also provides cerebral protection?
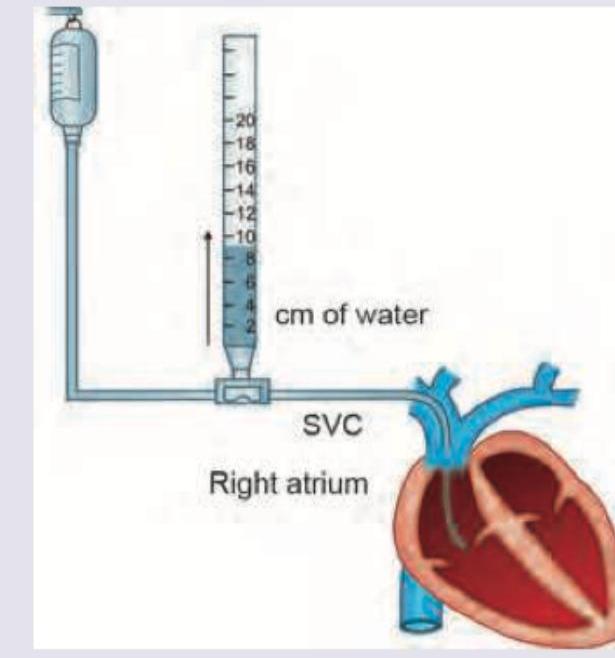
All are correct about the pressure recording shown below except: (Recent NEET Pattern 2016-17)
Most sensitive method of monitoring cardiovascular ischemia in the perioperative period is -
Which of the following is not used in controlling heart rate intraoperatively?
A patient with history of coronary artery disease presents with pulse rate of 48/min and low BP. Patient has decreased myocardial contractility on Echo. Which of these anesthetic agents is contraindicated?
Which of the following is not a cardiovascular monitoring technique
The most sensitive and practical technique for detection of myocardial ischemia in the perioperative period is -
Among the following anesthetic agents, portal vein flow is maximally reduced by:
Which drug is used for anesthesia in a hypotensive patient?
Practice by Chapter
Cardiovascular Physiology
Practice Questions
Anesthesia for Coronary Artery Disease
Practice Questions
Valvular Heart Disease Management
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Cardiopulmonary Bypass Principles
Practice Questions
Myocardial Protection Strategies
Practice Questions
Inotropes and Vasopressors
Practice Questions
Vasodilators in Cardiac Anesthesia
Practice Questions
Transesophageal Echocardiography
Practice Questions
Off-Pump Cardiac Surgery
Practice Questions
Management of Cardiac Pacemakers and ICDs
Practice Questions
Fast-Track Cardiac Anesthesia
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app