
Anesthetic Equipment and Monitoring — MCQs

On this page
The material used for a vaporizer should have which of the following qualities?
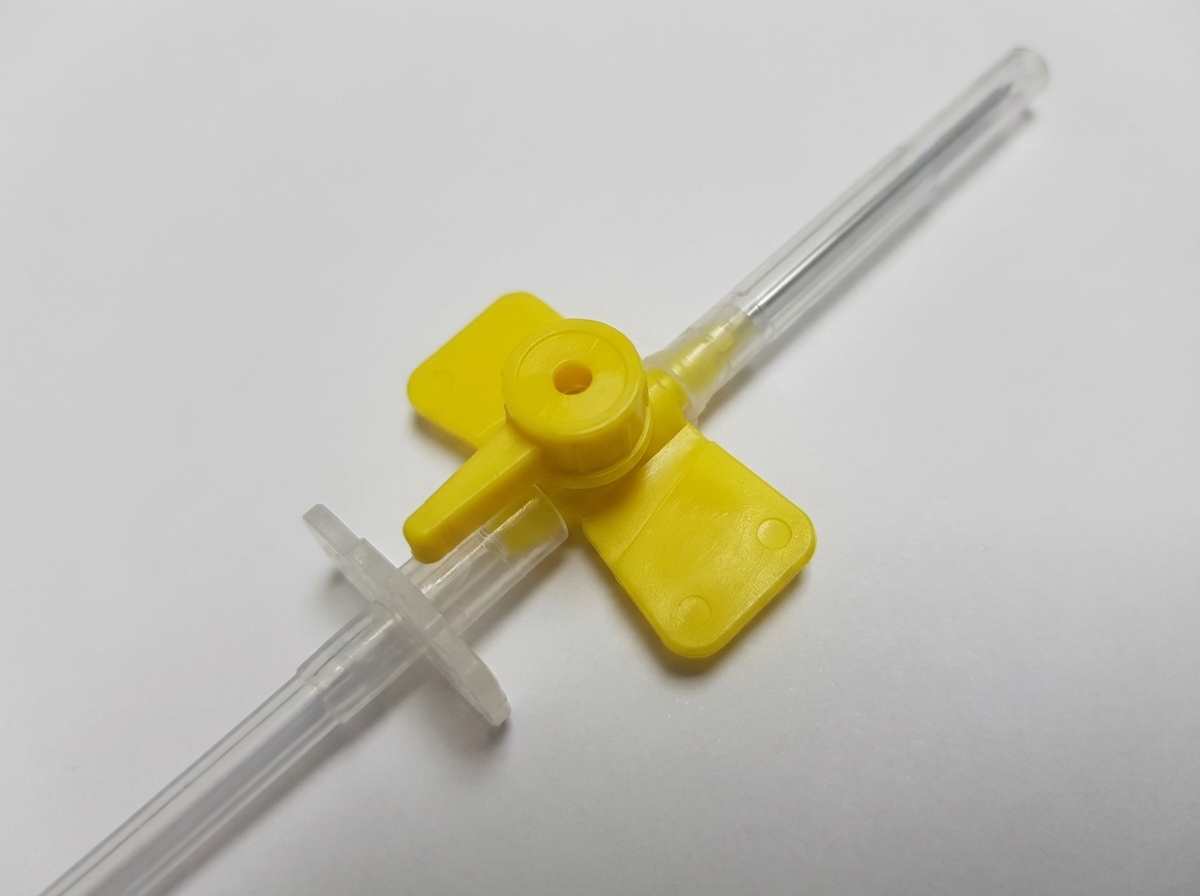
What is the primary use of the depicted device?

What is the name of the test performed before drawing an arterial blood gas sample?
Which of the following significantly decreases airborne infection in the operating room is NOT true?
Modern monitors to measure end-tidal CO2 (ETCO2) primarily utilize which principle?
What is the maximum oxygen concentration that can be attained with a Venturi mask?
What is the size of the intravenous cannula shown?
Which ECG lead is best for diagnosing arrhythmias during intraoperative monitoring?
Which of the following statements is NOT true regarding femoral artery cannulation?
Which of the following may result in a sudden increase in end-tidal CO2 (ETCO2)?
Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app