
Anesthetic Equipment and Monitoring — MCQs

On this page
Which of the following will produce decreased EEG activity?
Central line may be inserted in all of the following veins except?
What is a characteristic of an ideal gas?
In a typical blood gas analyser, which of the following is true?
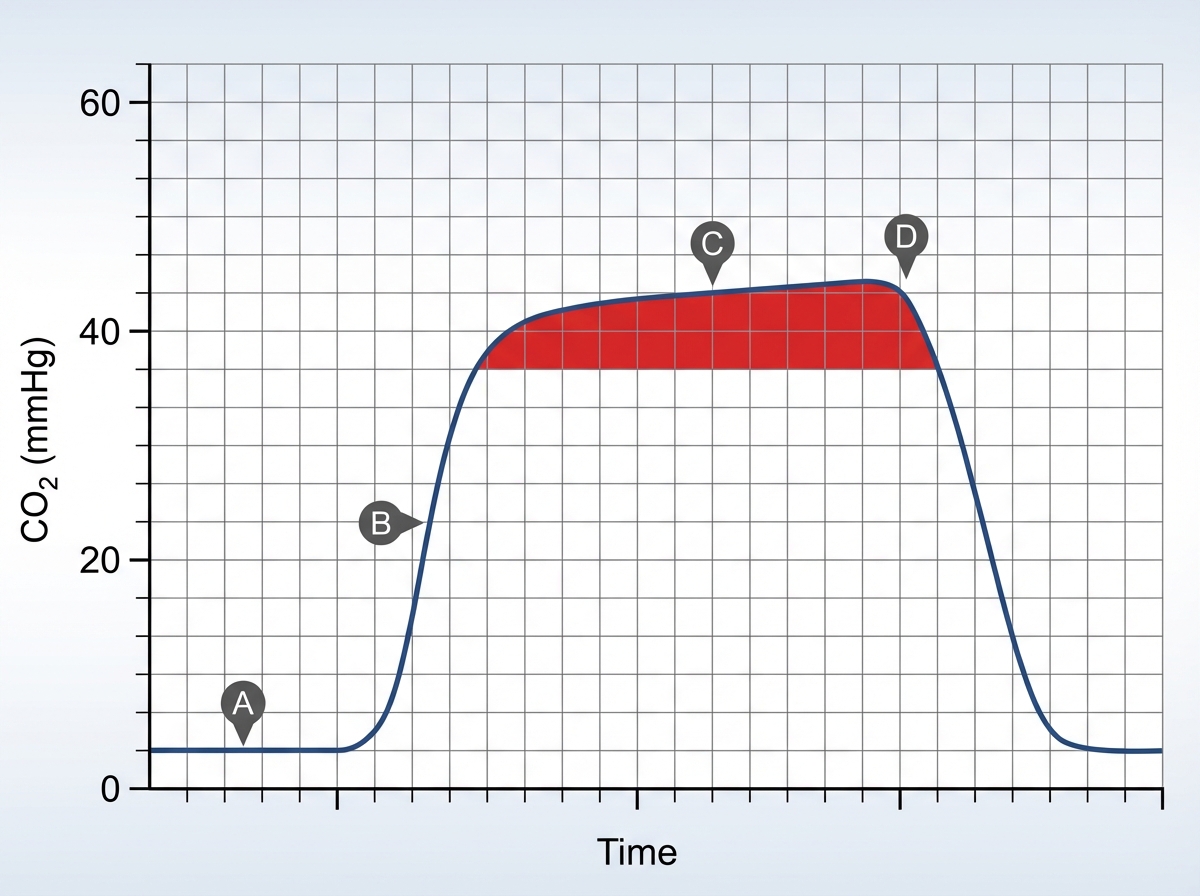
In the provided capnograph tracing, what does the red parameter represent?
Which cylinder size is most commonly used in an anesthesia machine?
What is the name of the following instrument?

What is the intraoperative use of the following device?

What is the modified shock index?
What is the colour coding of halothane, isoflurane, sevoflurane, and desflurane, respectively?
Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app