
Anesthetic Equipment and Monitoring — MCQs

On this page
What is the pressure at which oxygen is stored?
Which of the following inhalational agents sensitizes myocardium to catecholamines
What does the acronym DISS stand for in the context of medical gas supply?
Identify the mask used for patients requiring high concentrations of oxygen.

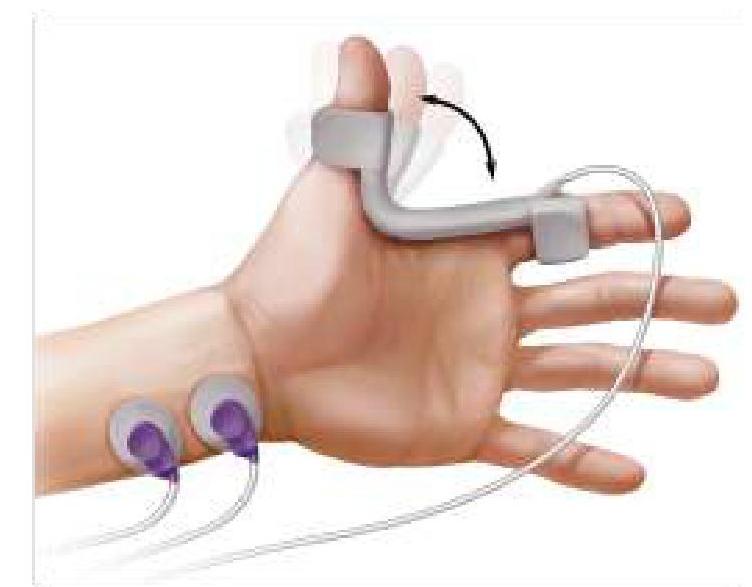
The image given below shows neuromuscular monitoring of the patient after anesthesia. What is the most commonly used nerve for monitoring?
Which of the following is the most commonly used objective method for monitoring depth of anaesthesia in modern practice?
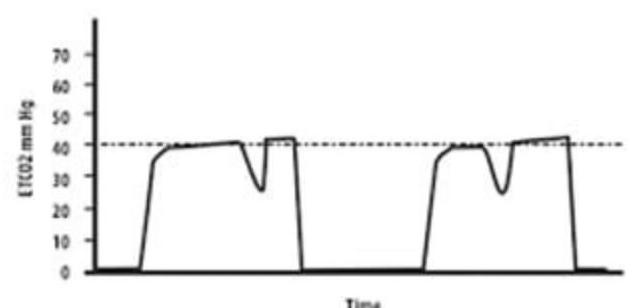
What does the image of the Capnograph depict?
Which anesthetic gas is known for causing maximum respiratory irritation?
Which is the most effective circuit in spontaneous anaesthesia?
What is the purpose of Murphy's eye in an endotracheal tube?
Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app