
Anesthetic Equipment and Monitoring — MCQs

On this page
Most anesthetic drugs are detectable by entropy monitoring, except:
What happens to end-tidal carbon dioxide (ETCO2) when the rate and depth of breathing are increased?
Which of the following is a fixed performance device?
100 grams of soda lime absorbs what percentage of CO2?
Which of the following endotracheal tubes features a high-pressure, low-volume cuff?
Which of the following is used to measure the depth of anesthesia?
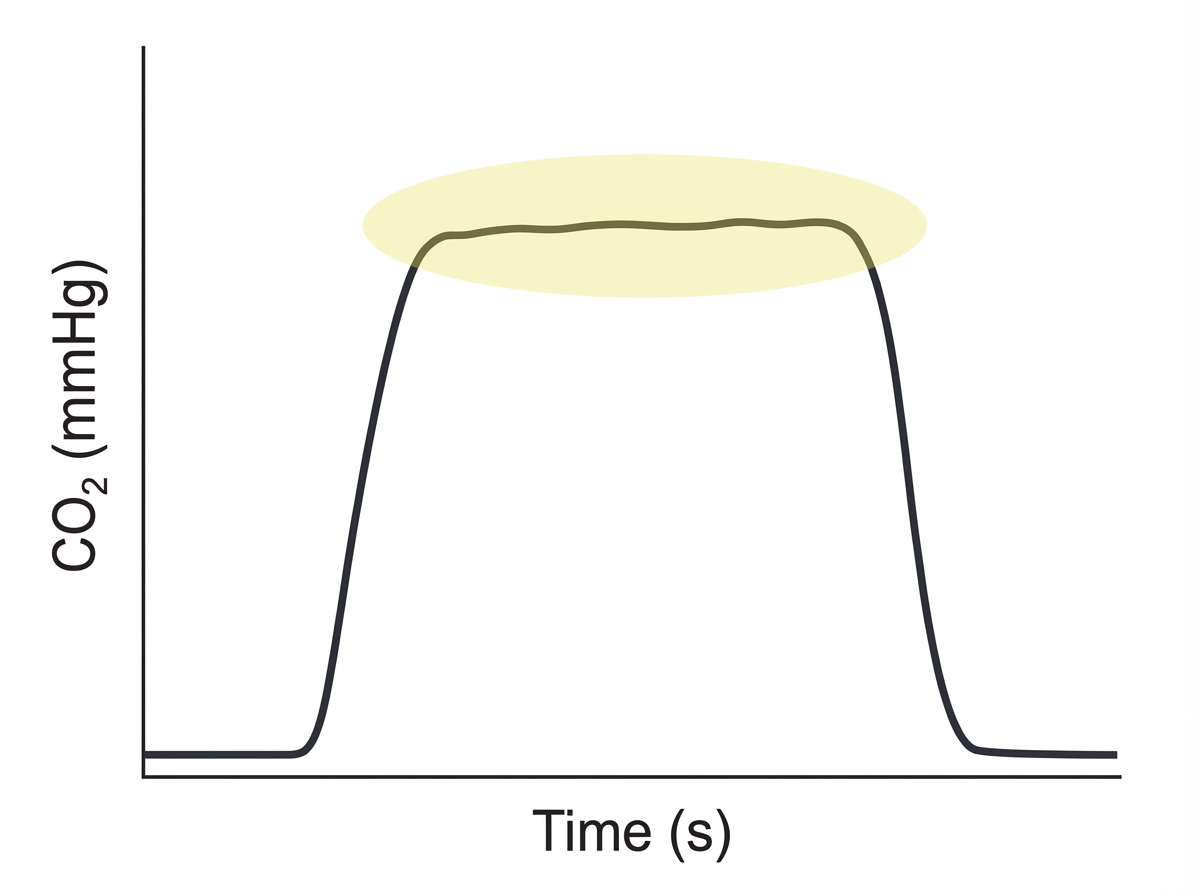
The circled part of the given capnograph reflects which of the following?
What is the standard color of an oxygen cylinder?
Which of the following non-invasive methods is used in detecting the position of tubes during ventilation?
All are constituents of soda lime except?
Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app