
Anesthetic Equipment and Monitoring — MCQs

On this page
What does the marking $X$ in the endotracheal tube indicate? (Recent NEET Pattern 2016-17)

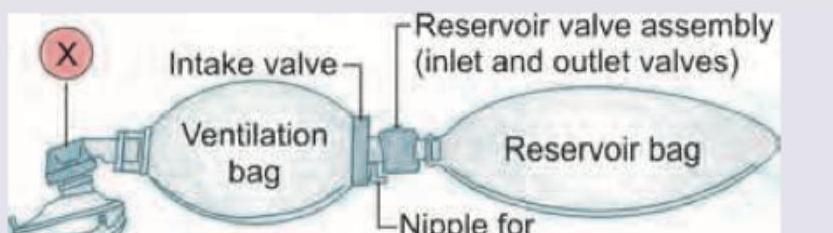
The resuscitation breathing system shown below has a valve regulating flow of fresh gas to the patient. This valve marked as $X$ is
Which is correct about the laryngoscope blades shown below? (Recent NEET Pattern 2016-17)

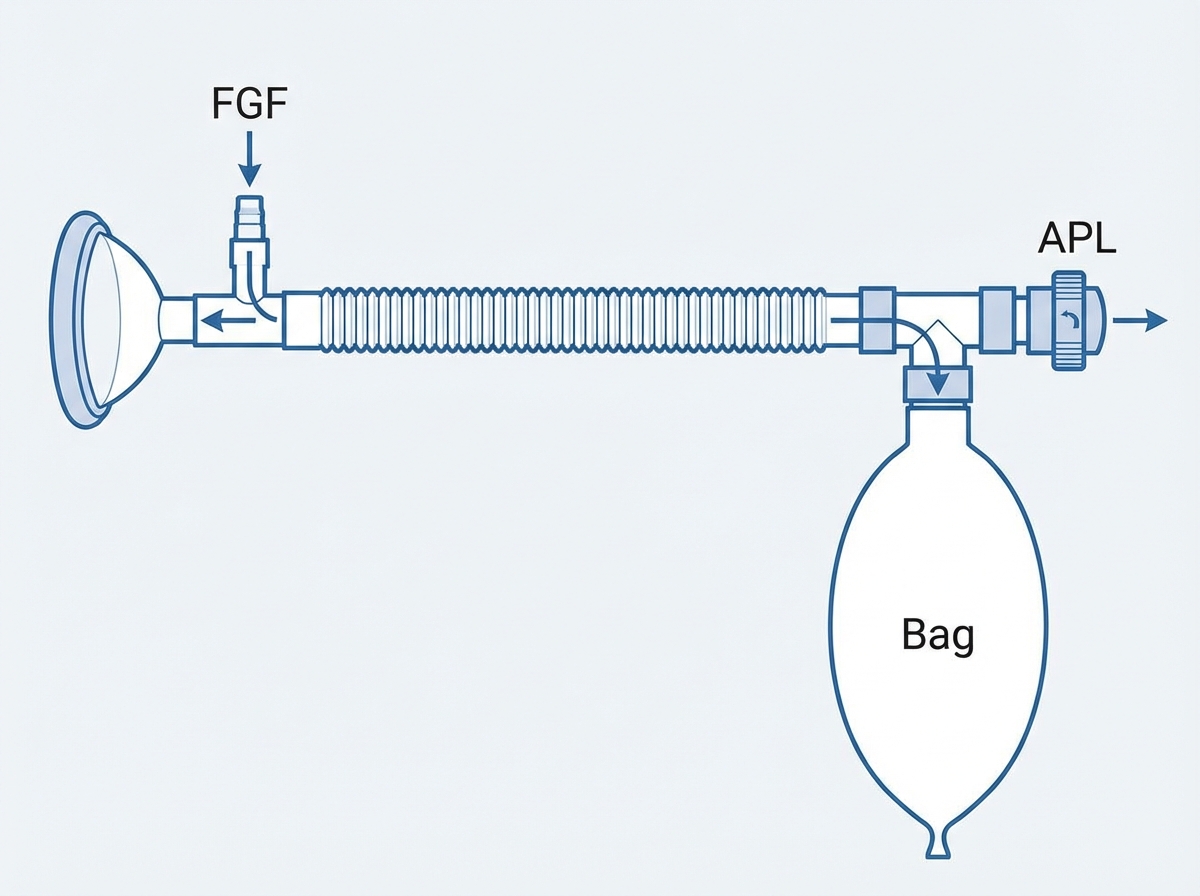
What is the following circuit known as?
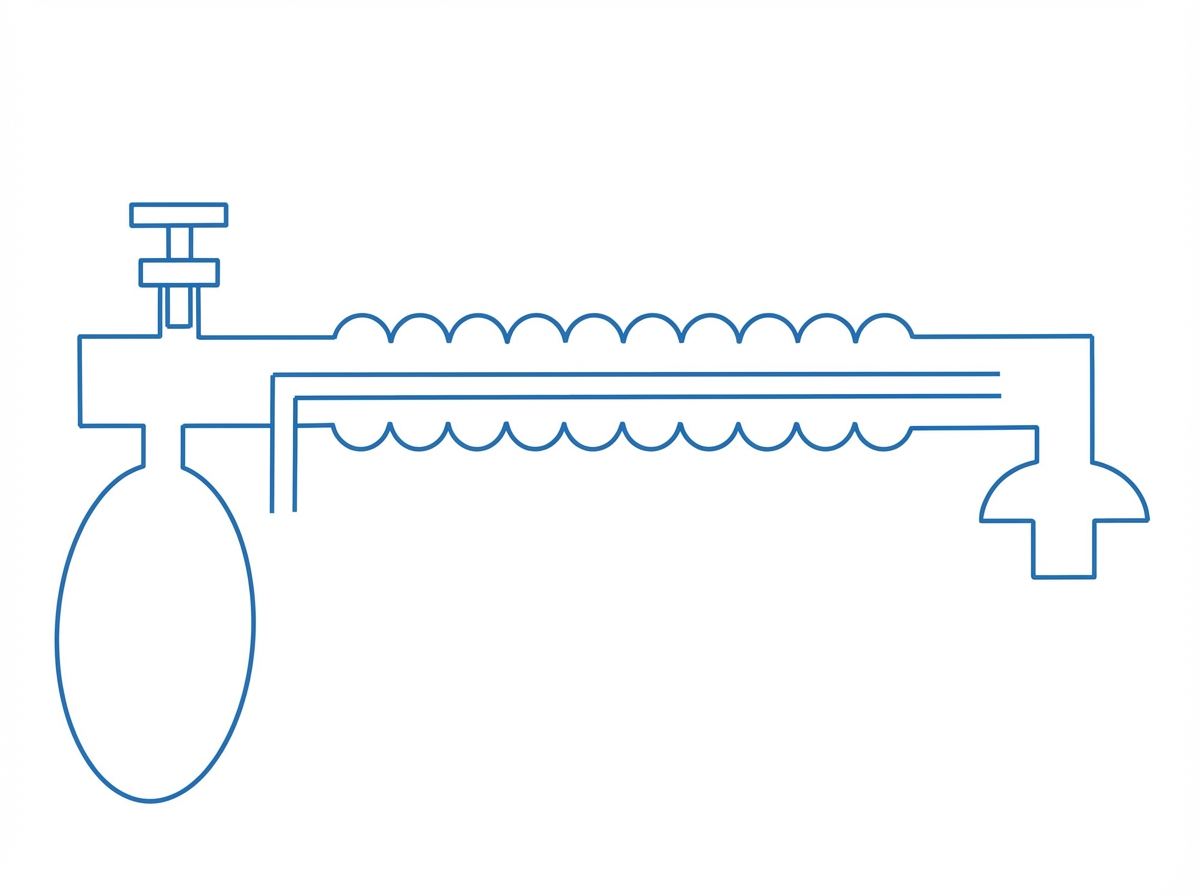
Which of the following Mapleson system is shown below?
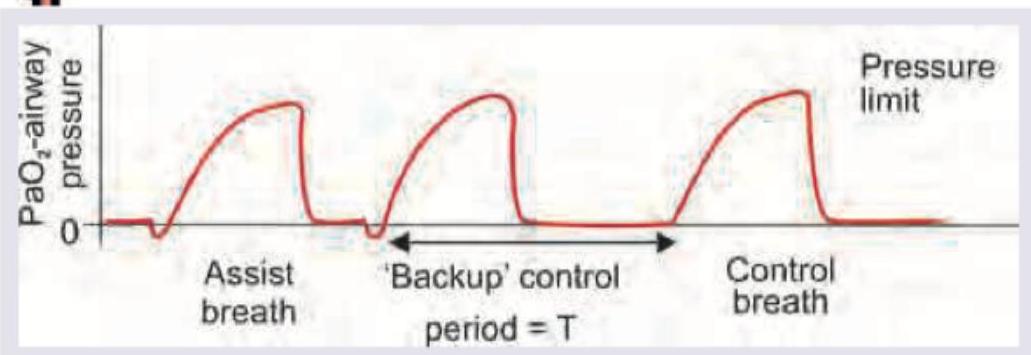
What is the mode of ventilation shown here?
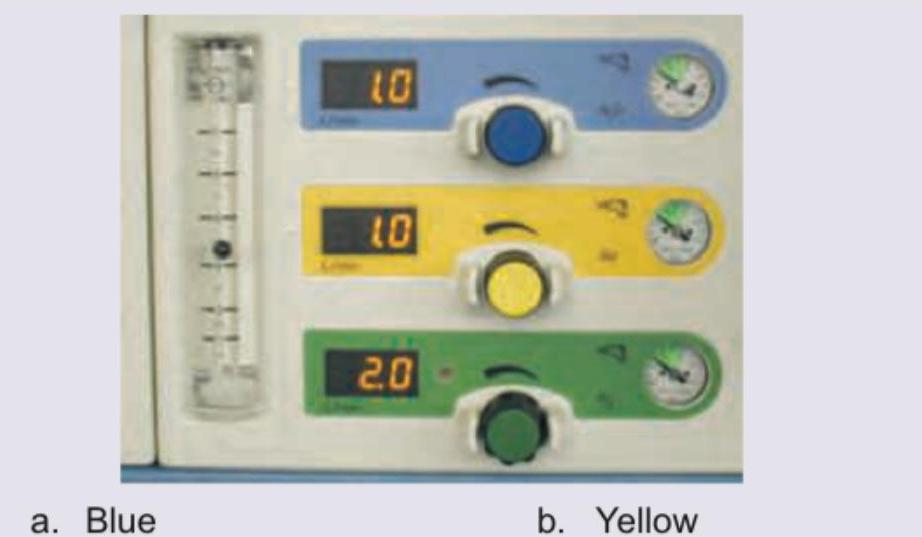
Which of the knobs shown below represent the knob controlling oxygen flow in the anesthesia machine?
The following drug is colour coded for perioperative use:

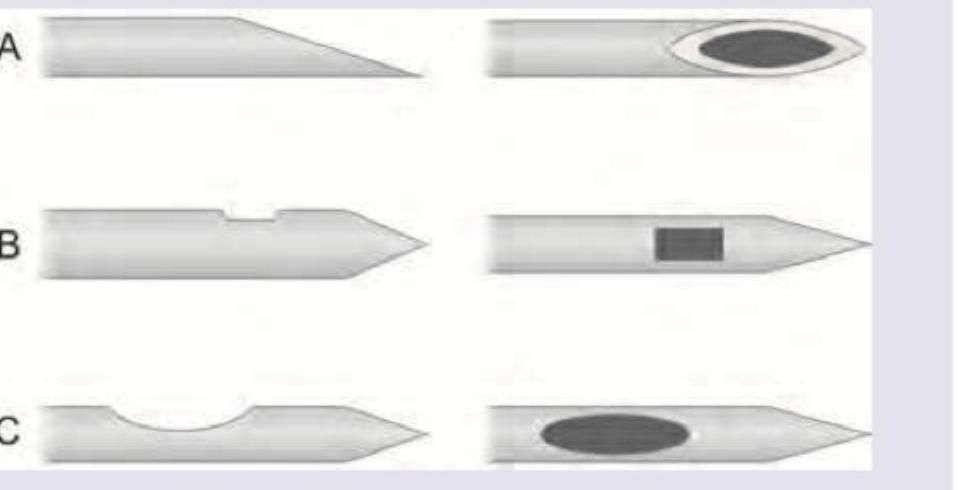
(1) Identify the spinal needles shown in the image:
Maximum oxygen concentration can be delivered by:
Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app