
Anesthetic Equipment and Monitoring — MCQs

On this page
What is the minimum mandatory percentage of oxygen used in general anaesthesia?
Which of the following may result in a sudden increase in end-tidal carbon dioxide (ETCO2)?
What is the normal Central Venous Pressure (CVP)?
A 60-year-old female patient underwent modified radical mastectomy under general anesthesia. She is very anxious preoperatively. What monitor might the anesthetist have used during surgery to ensure she does not recall intraoperative events?
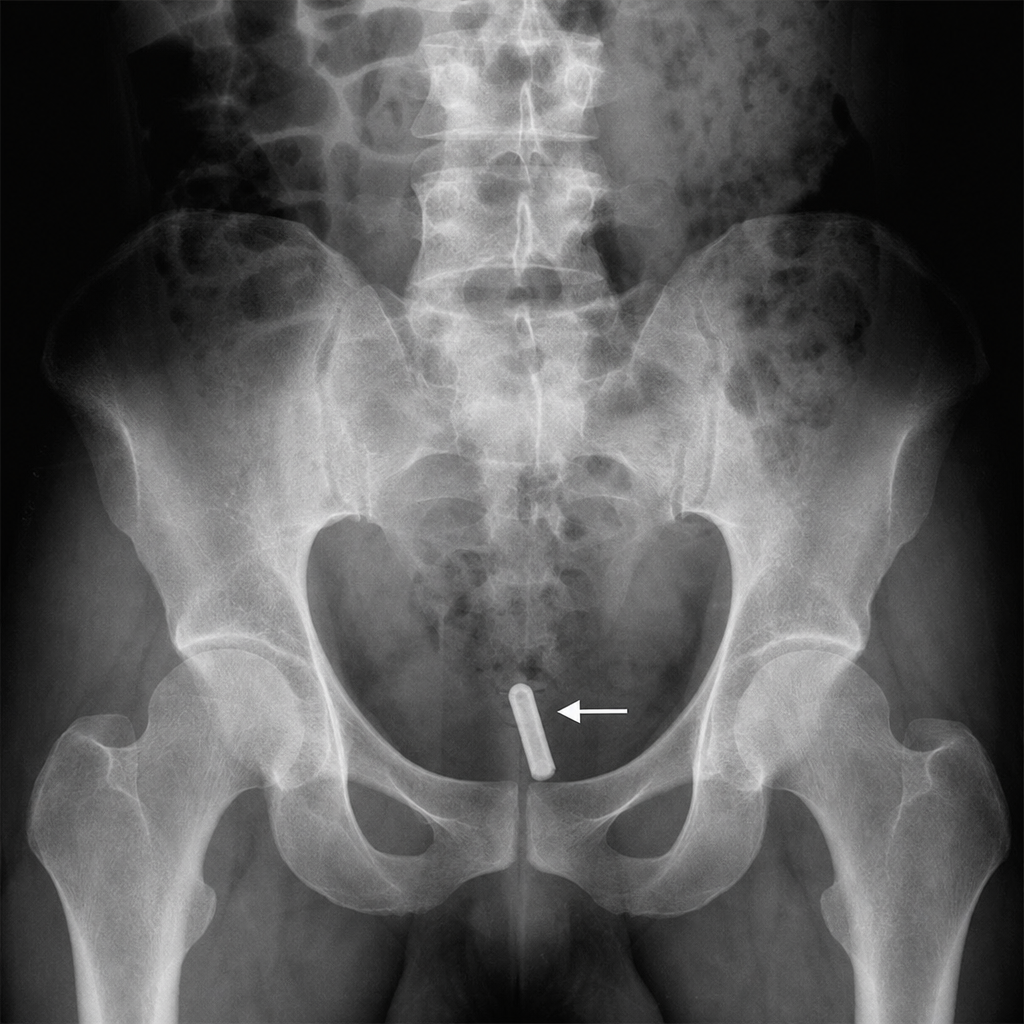
The image shows an endotracheal tube with an arrow pointing to a specific component near the bevel. Which of the following best describes the location and function of the marked component?
Which pattern of capnograph is indicative of endotracheal tube obstruction?
Ayer's T Piece is classified as which of the following Mapelson circuits?
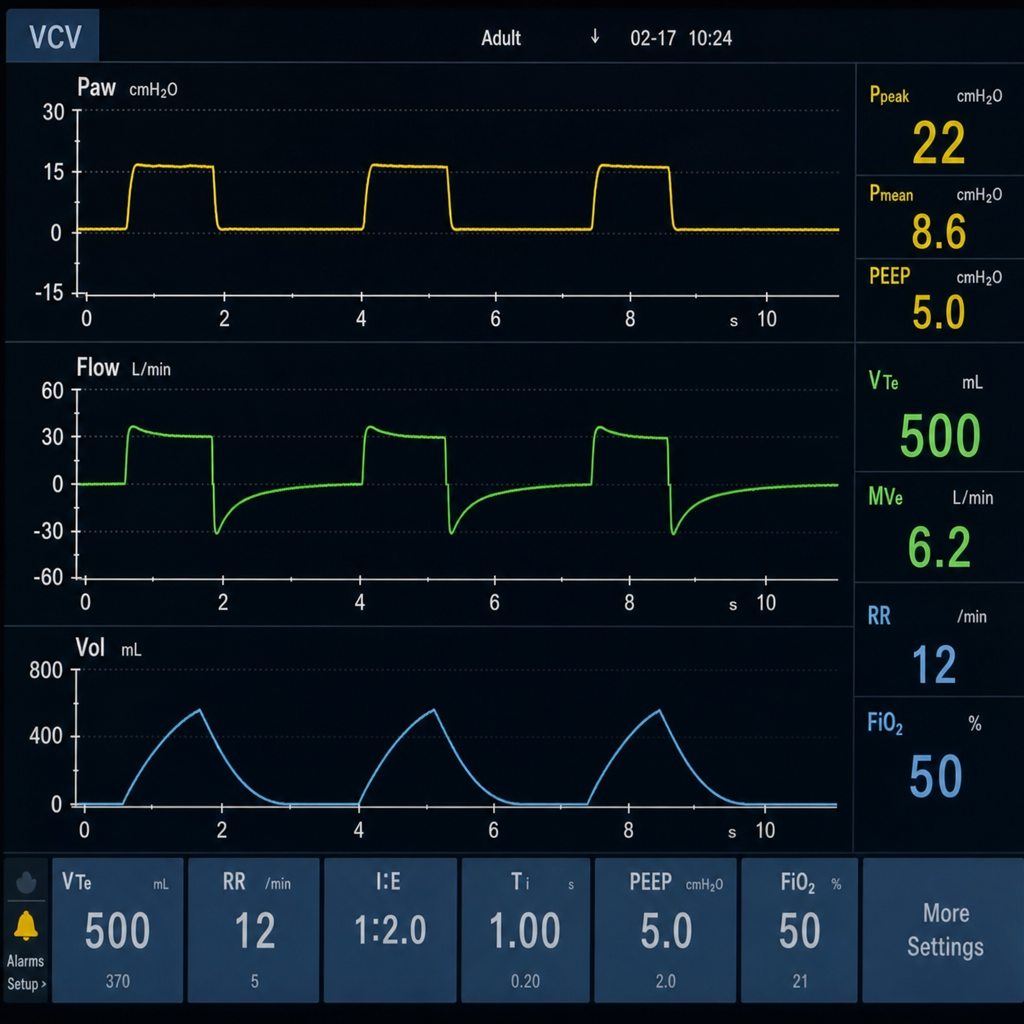
This type of flow-time graph is typically observed in which mechanical ventilator mode?
Which size cannula is typically used for massive bleeding during surgery?
During a liver transplant, a patient develops prolonged bleeding. The anesthesiologist uses the coagulation analyzer shown in the image to guide management. Which parameter measured by this device would most likely be critically abnormal in a patient with hepatic synthetic dysfunction, explaining the bleeding?

Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app