
Anesthetic Equipment and Monitoring — MCQs

On this page
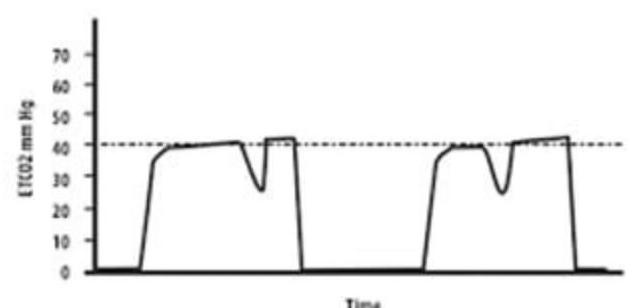
What does the image of the Capnograph depict?
What is the purpose of Murphy's eye in an endotracheal tube?
Which nerve is commonly tested to assess the adequacy of anaesthesia?
Which is the most effective circuit in spontaneous anaesthesia?
What is the composition of soda lime?
What is the PRIMARY application of capnography during patient monitoring?
Critical temperature of oxygen is?
Circuit of choice for controlled ventilation ?
Critical temperature for liquid nitrogen is ?
In which vein is Central Venous Pressure (CVP) most accurately monitored?
Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app