
Anesthetic Equipment and Monitoring — MCQs

On this page
A sevoflurane vaporizer can accurately deliver the dose of an anesthetic agent. This accuracy depends on which of the following properties of the anesthetic agent?
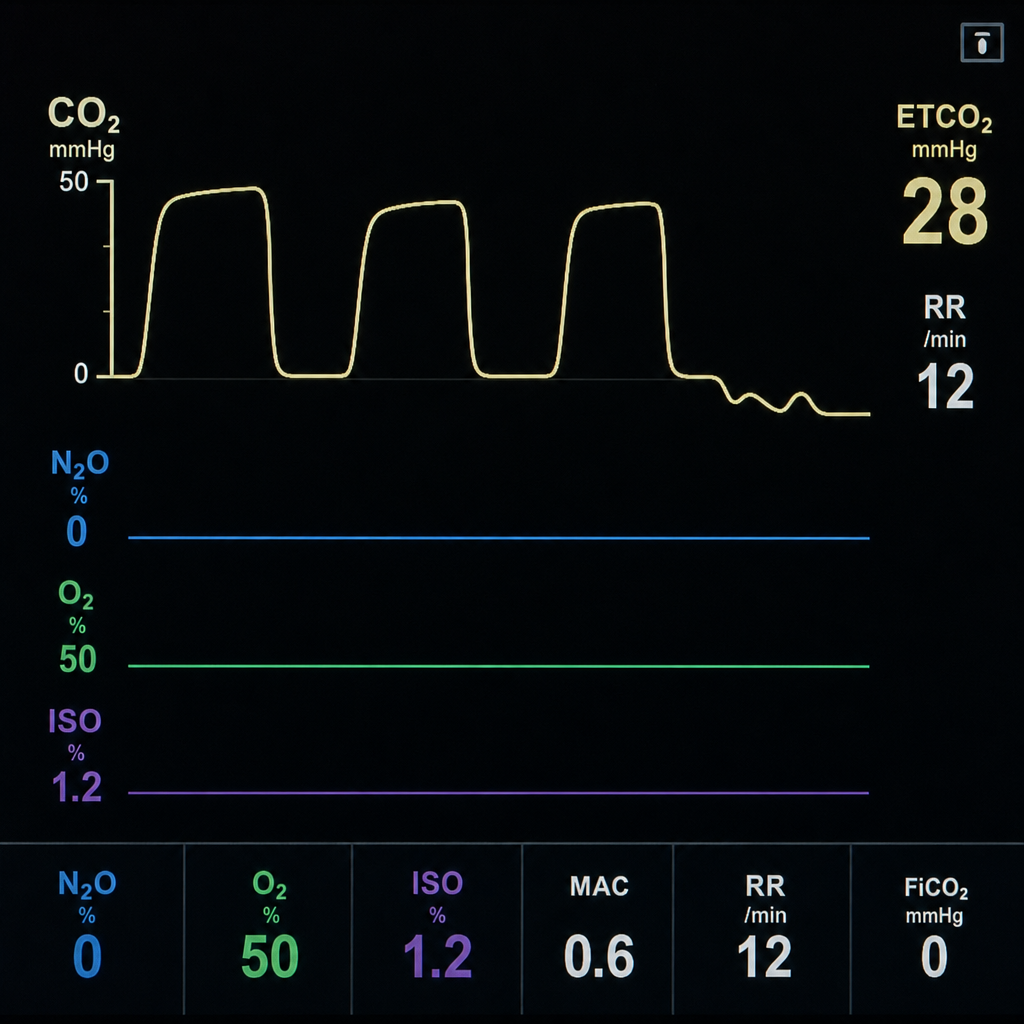
During intraoperative period following capnograph waveform is seen. What does it signify.
Depth of Anesthesia is best measured by:
Neuromuscular monitoring shows TOF ratio 0.7. This indicates:
In a patient undergoing surgery with significant blood loss, which parameter is monitored using TEG or ROTEM?
What is the significance of monitoring central venous pressure (CVP) during major surgery?
What is the primary function of the vaporizer in an anesthesia machine?
During major surgery, a patient is monitored using ROTEM. The results show reduced clot firmness and increased clotting time. Which treatment should be administered to correct these abnormalities?
Which of the following statements about Wright's spirometer is true?
Which of the following is the most common method used to know depth of anaesthesia?
Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app