
Anesthetic Equipment and Monitoring — MCQs

On this page
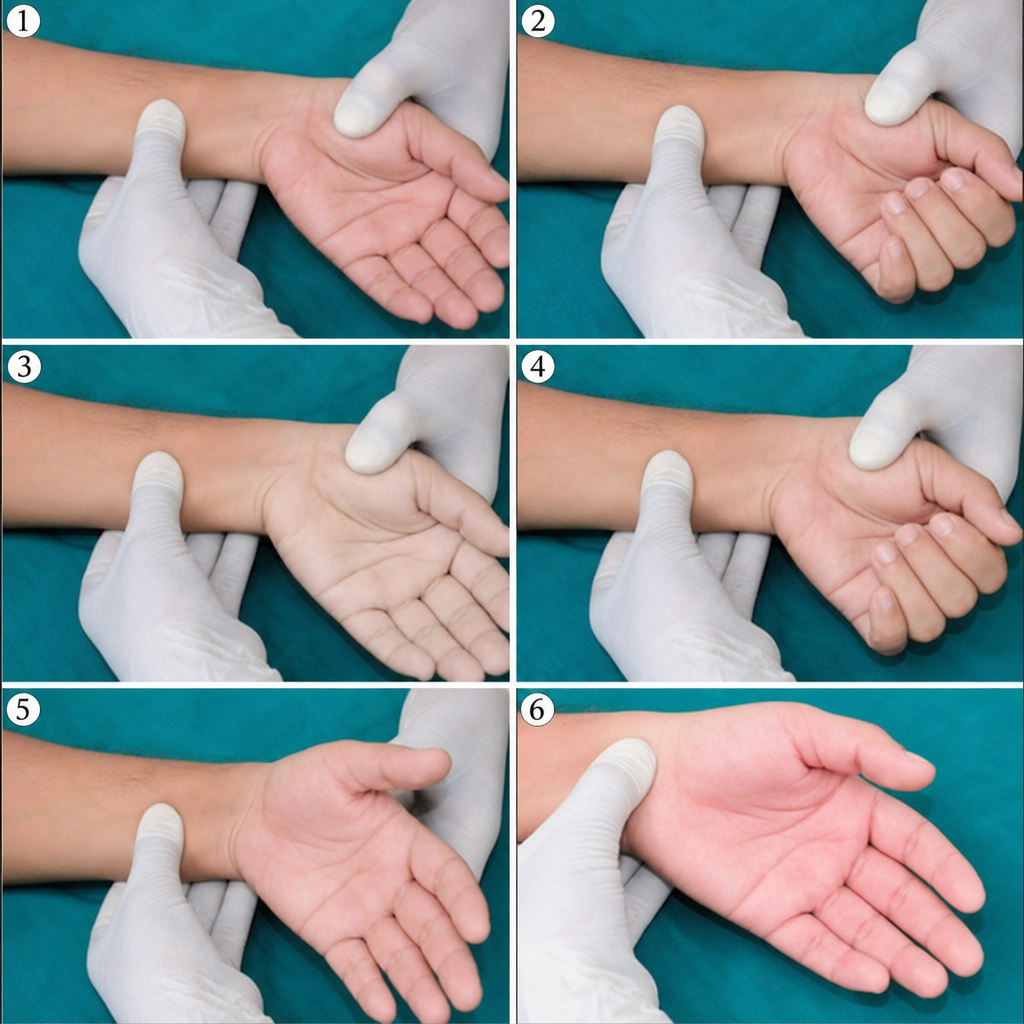
Which collateral-circulation test may be performed before radial artery puncture for ABG sampling:
The Penaz technique:
All true about interaction of SpO2 reading and methemoglobinemia, except:
If an anesthetist at high altitude uses plenum vaporizers, what will be the delivered vapor concentration?
Gas cylinder with single pin index ?
A 25 year old male is undergoing incision and drainage of abscess under general anaesthesia with spontaneous respiration. Which of the following is the most efficient anaesthetic circuit which can be used in this patient?
The pulse oximetry reading is affected in:
The Pin Index Safety System (PISS) number for nitrous oxide (N2O) is
According to standard medical gas cylinder color coding, the colour of ethylene cylinder is:
Early and reliable indication of air embolism during anaesthesia can be obtained by continuous monitoring of:
Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app