
Anesthetic Equipment and Monitoring — MCQs

On this page
The image shows an Ambu SPUR II adult Bag-Valve-Mask resuscitator with its pressure-relief (Pop-Off) valve. What is the pressure required to open this pressure-relief valve?

Which of the following is the best method to assess the degree of muscle relaxation?
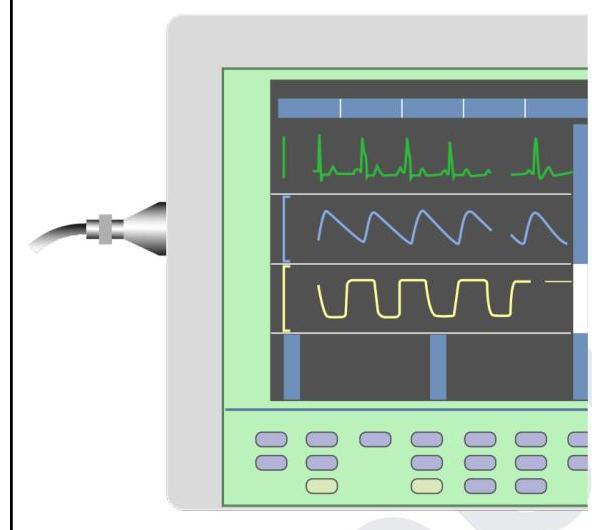
You are in the operating room and notice the tracing in yellow colour on this device. What does it indicate?
What is the color of the nitrous oxide cylinder?
In which of the following carbon dioxide absorbents is water used for hardening?
A 20-year old spontaneous breathing patient undergoing incision and drainage under GA, which of the following is the breathing circuit of choice for spontaneous ventilation?
True statement regarding pin index:
As per ISO, color of N2O cylinder is –
What is defined as recovery index of the neuromuscular blocker (NMB):-
Depth of anaesthesia can be best assessed by
Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app