
Anesthetic Equipment and Monitoring — MCQs

On this page
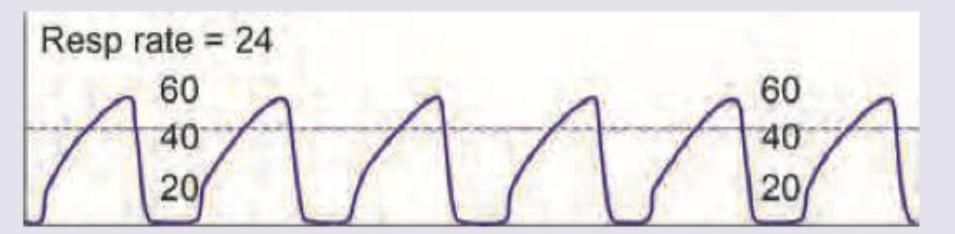
The capnography image shows:
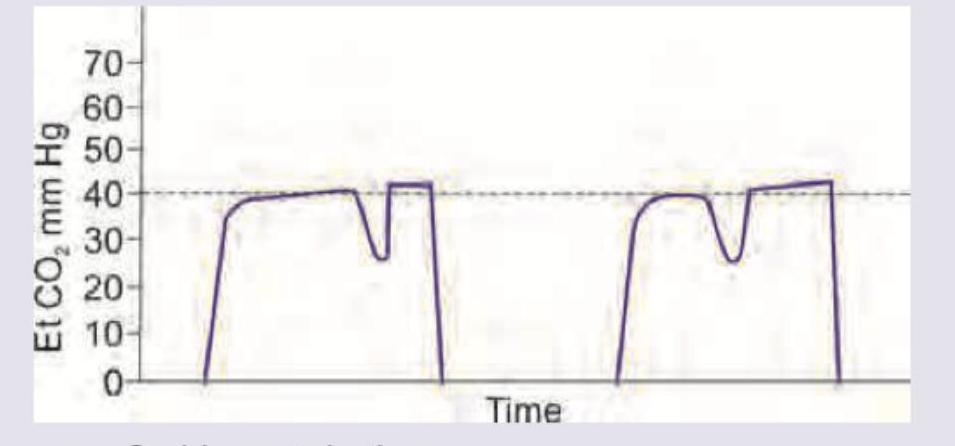
A patient is undergoing abdominal surgery under general anesthesia with controlled mechanical ventilation, and complete neuromuscular blockade is required for the procedure. The following capnography tracing is observed. What is the next best step?
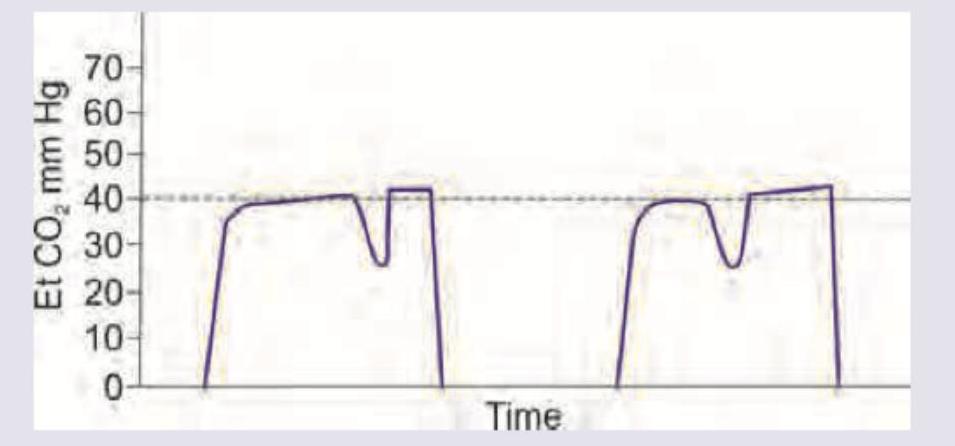
What does the following capnographic recording represent?
The image shows capnography recording. Et CO2 is measured at:
What does the marking $X$ at endotracheal tube indicate? (Recent NEET Pattern 2016-17)

What does the marking $X$ in the endotracheal tube indicate? (Recent NEET Pattern 2016-17)

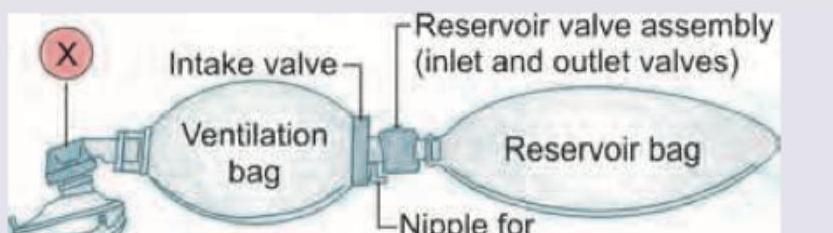
The resuscitation breathing system shown below has a valve regulating flow of fresh gas to the patient. This valve marked as $X$ is
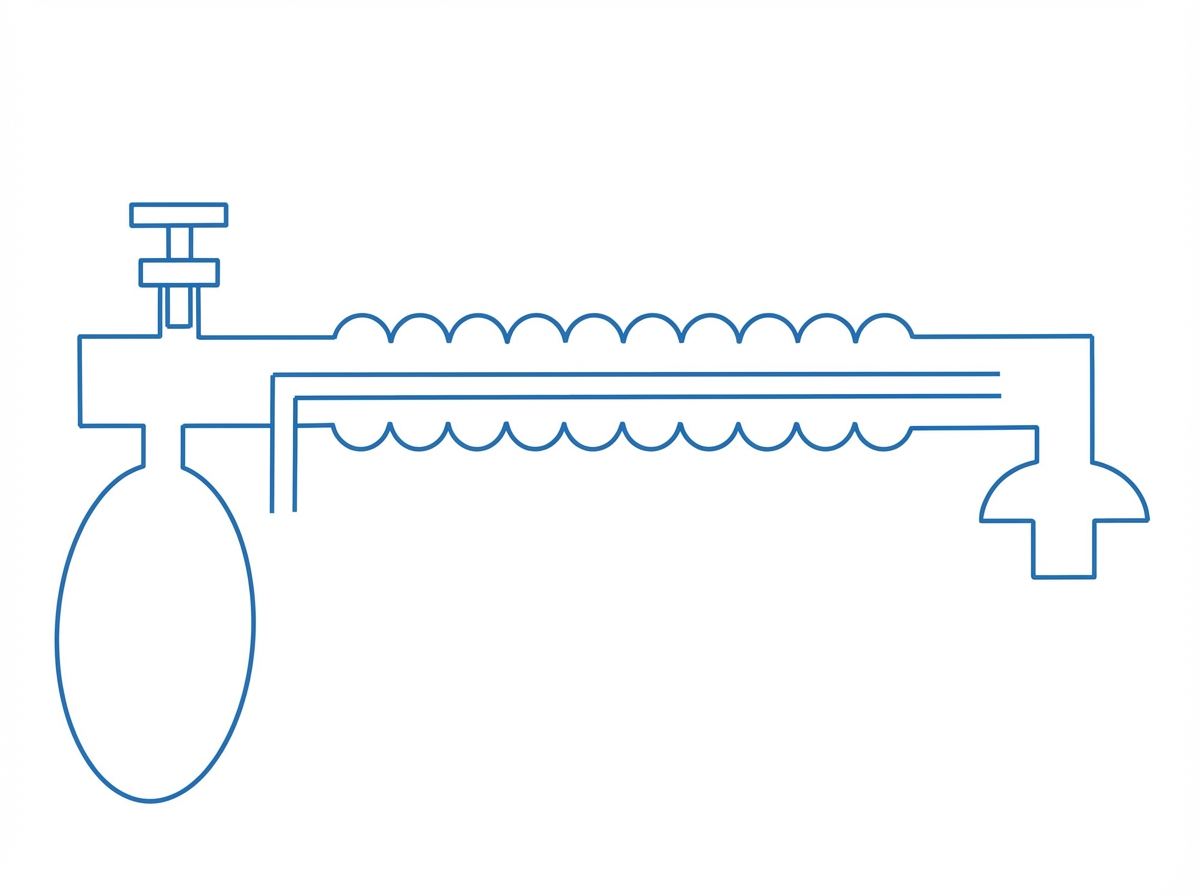
What is the following circuit known as?
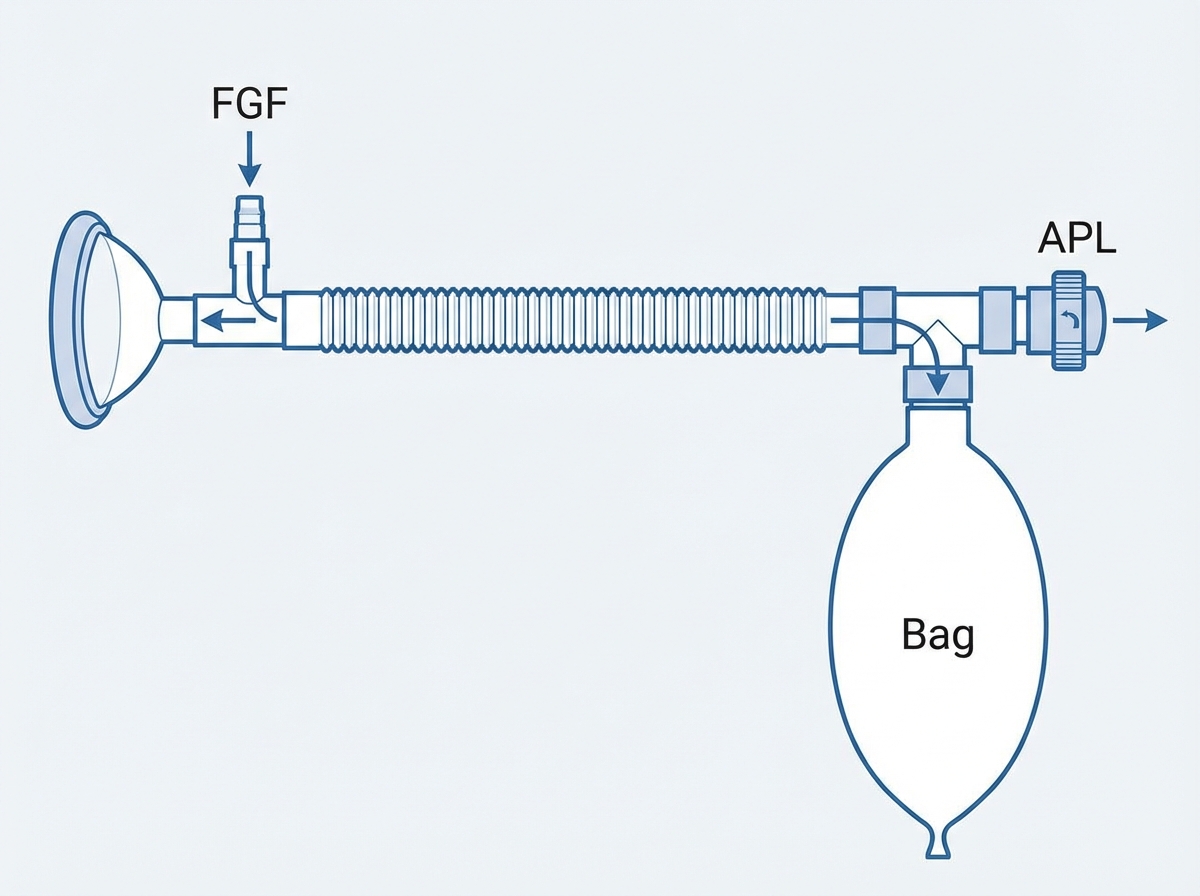
Which of the following Mapleson system is shown below?
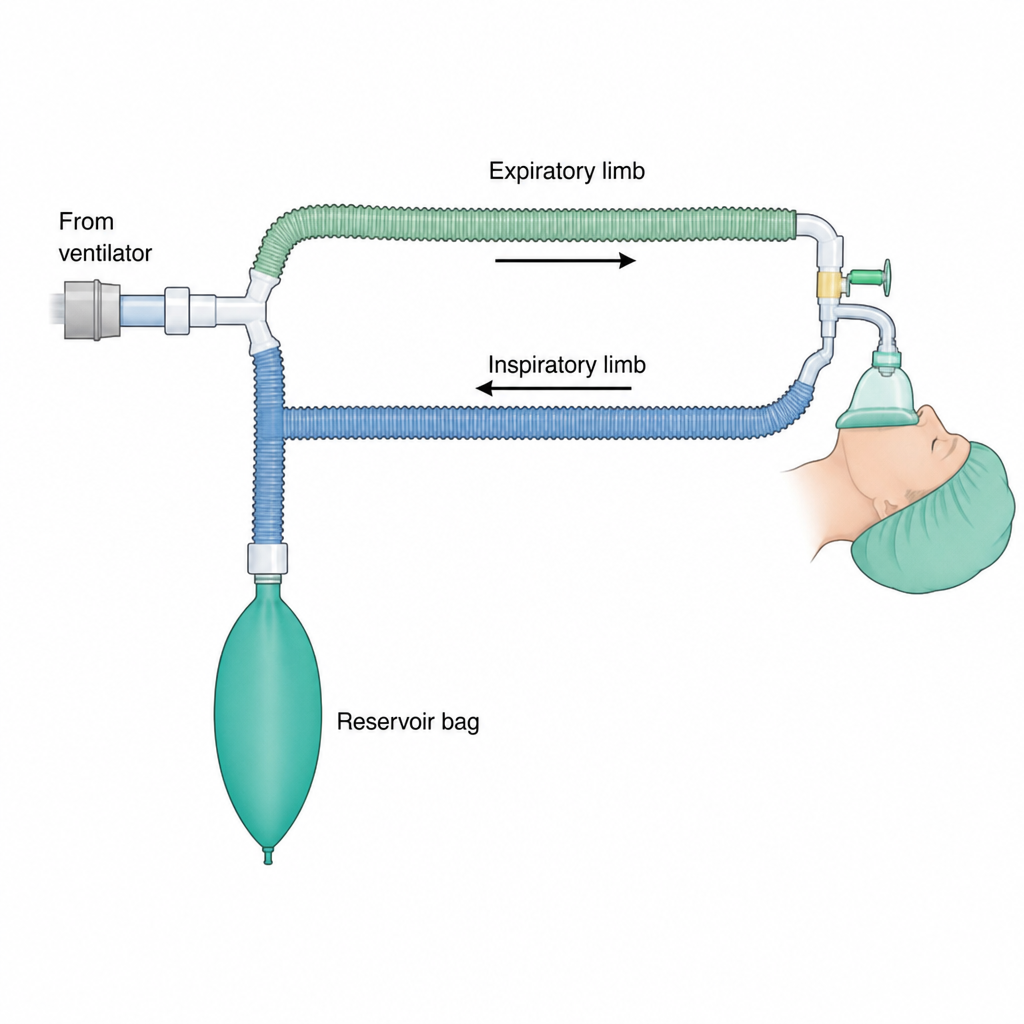
Which of the following Mapleson system is shown below?
Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app