
Anesthetic Equipment and Monitoring — MCQs

On this page
All of the following sites are used for intraosseous access (the route shown below) except:

The pin index of the following nitrous oxide cylinder (blue color per ISO 32:1977 standard) is:

A nitrous oxide cylinder is shown. What is its pin index?

A young intern is managing a patient of Acute MI who developed cardiac arrest when thrombolysis was initiated. The patient was intubated, CPR was performed and one ampoule of adrenaline was given. The capnographic tracing indicates:
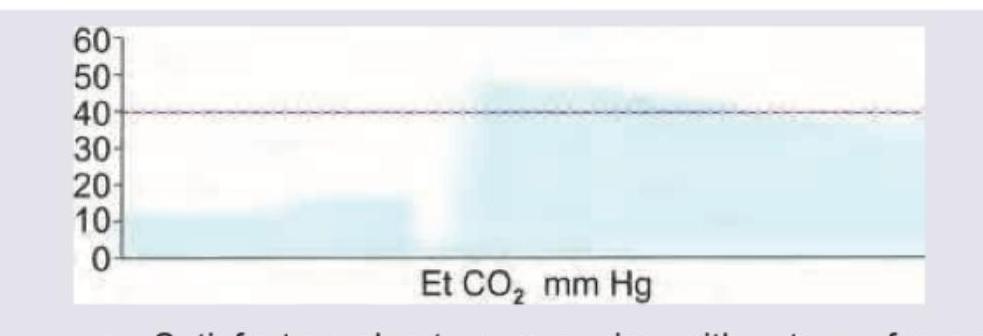
The following capnographic tracing shows:
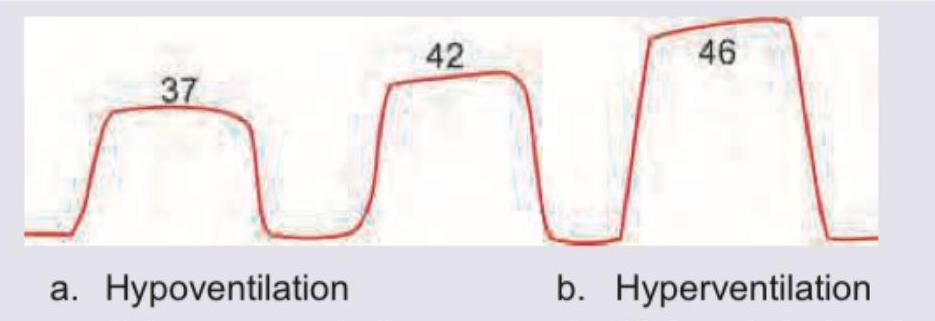
A mechanically ventilated patient has their respiratory rate increased from 12 to 20 breaths/min with stable hemodynamics and unchanged metabolic status. The following capnographic tracing represents:
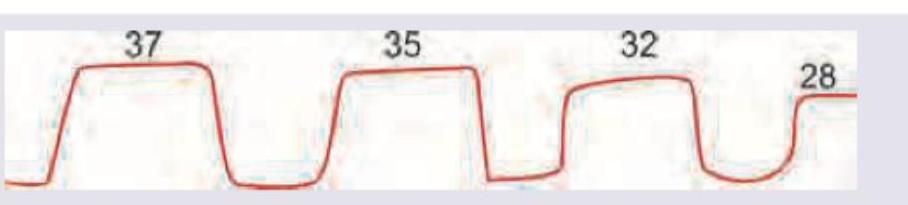
The following capnographic tracing represents:
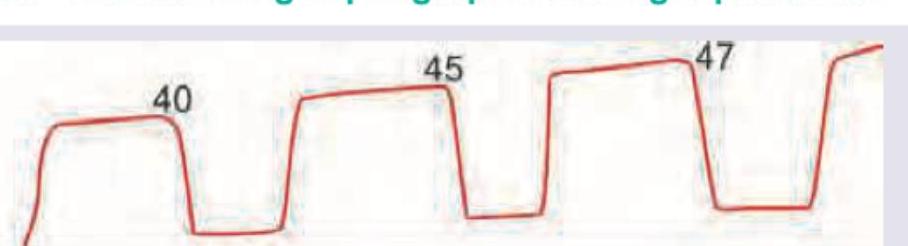
The following capnographic tracing represents:
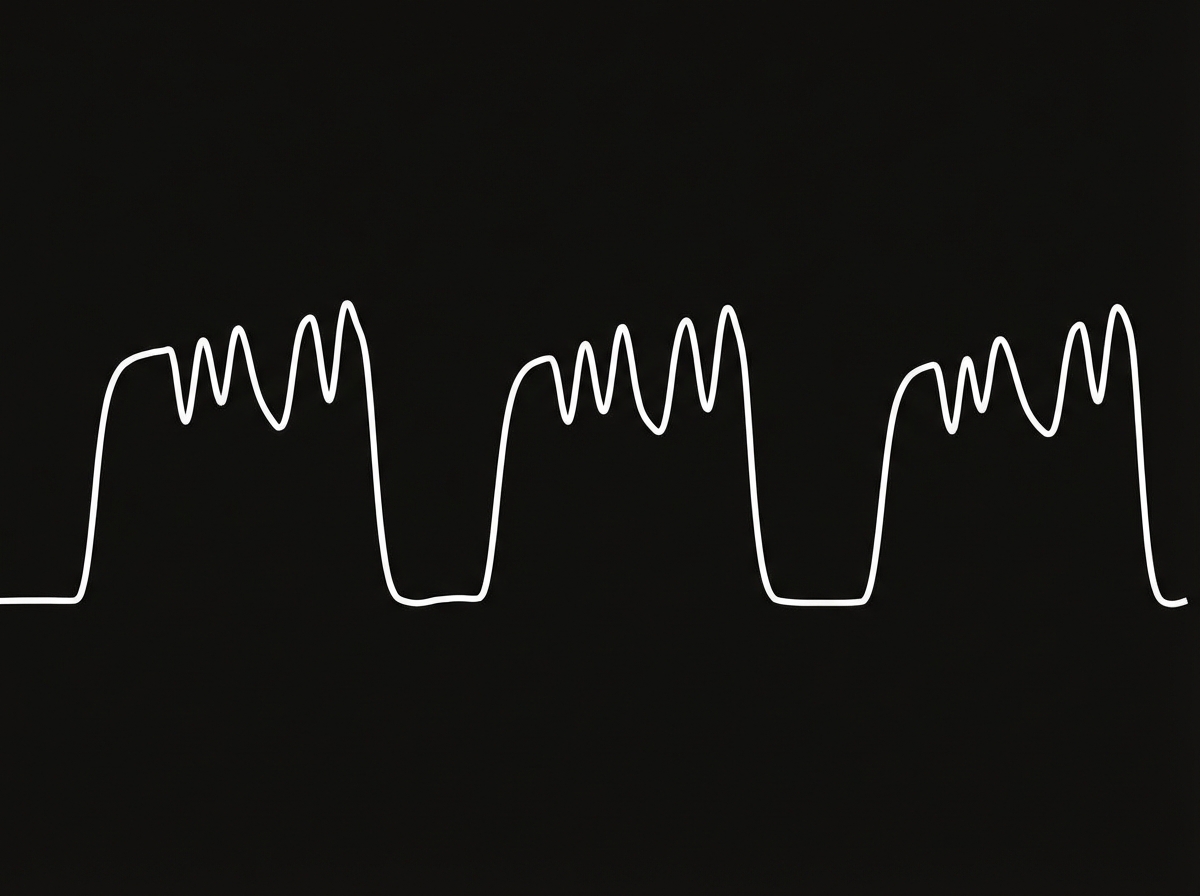
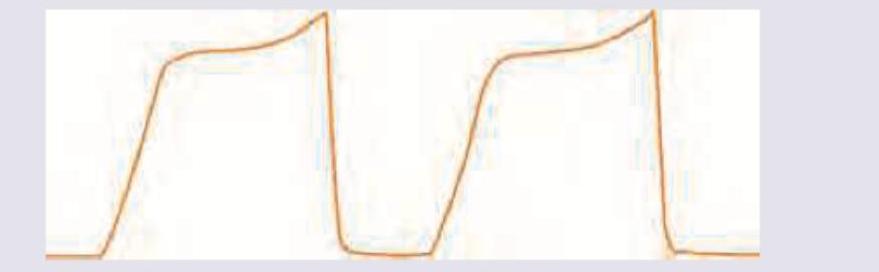
The following capnographic tracing is seen in:
The interpretation for the following capnography is:

Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app