
Anesthetic Equipment and Monitoring — MCQs

On this page
You are administering anesthesia in a location that does not have an oxygen supply line. The E-cylinder that you are using reads 500 psig. Your oxygen flows are 10 L/min. Approximately how long does it take for your E-cylinder to empty?
Regarding variable orifice flowmeters, which statement is true?
Henry's law states that?
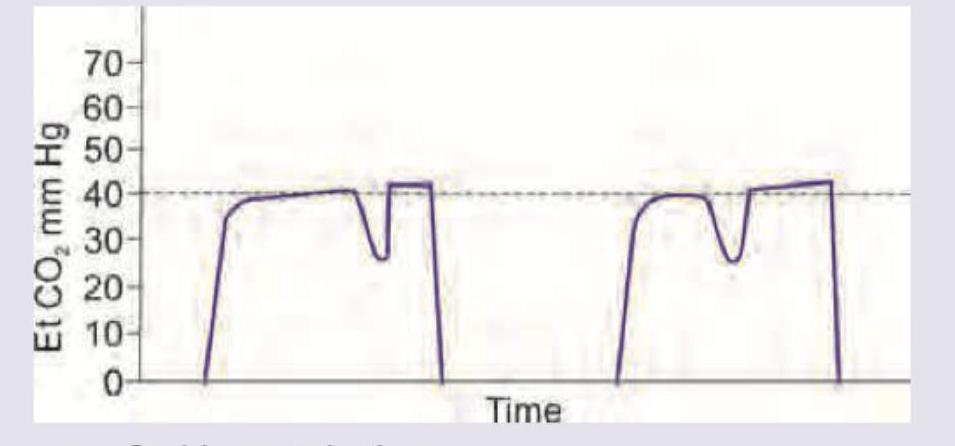
The provided capnography (ETCO2) curve depicts which of the following conditions?
Which modality is best utilized for neuromuscular monitoring during the maintenance of anesthesia?
What is the most sensitive method for non-invasive monitoring of cardiovascular ischemia in the perioperative period?
Central venous pressure (CVP) and pulmonary wedge pressure provide an accurate assessment of all of the following EXCEPT?
What is true about Nitrous Oxide (N2O)?
All of the following are safety measures to prevent the delivery of a hypoxic gas mixture to the patient, except –
What are the most frequently reported malfunctions in medical gas pipeline systems?
Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app