
Anesthetic Equipment and Monitoring — MCQs

On this page
A patient undergoing surgery shows a sudden drop of end -tidal CO₂ (ETCO₂) to zero on capnography. What does this most likely indicate?
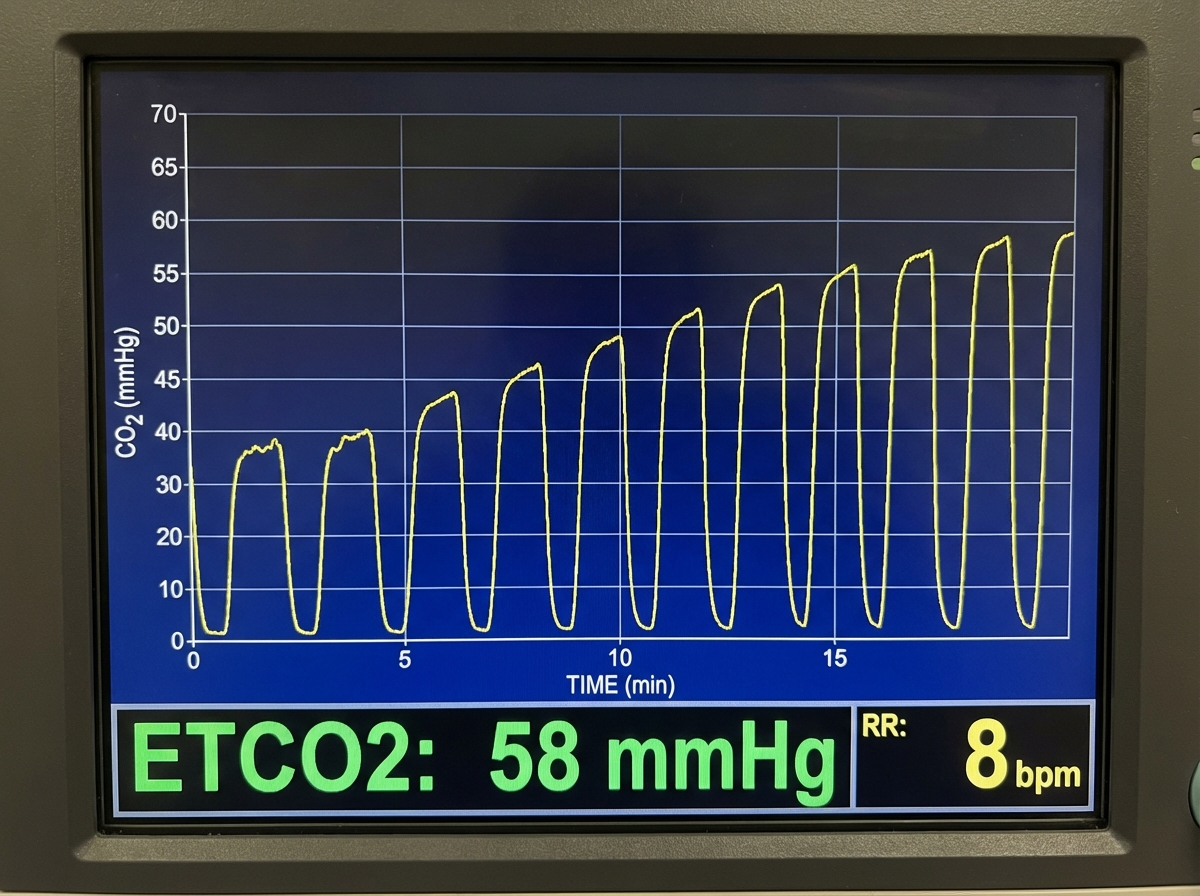
Which of the following conditions is NOT associated with the shown graph?
Which of the following tubes is used in surgery for cleft palate repair?
Bains' circuit is which type of Mapleson circuit?
What is the most sensitive investigation for air embolism?
Practice by Chapter
Anesthesia Machine Components
Practice Questions
Breathing Systems
Practice Questions
Vaporizers
Practice Questions
Gas Cylinders and Pipeline Supply
Practice Questions
Anesthesia Ventilators
Practice Questions
Standard Monitoring: ECG, BP, Pulse Oximetry
Practice Questions
Capnography
Practice Questions
Neuromuscular Monitoring
Practice Questions
Temperature Monitoring
Practice Questions
Invasive Hemodynamic Monitoring
Practice Questions
Equipment Troubleshooting
Practice Questions
Safety Features in Modern Anesthesia Equipment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app