
Upper Limb — MCQs

On this page
Which nerves primarily supply the small muscles of the hand?
What is the nerve supply of the structure marked in the image?

The image shows a highlighted region on the dorsal aspect of the hand (anatomical snuffbox). Which of the following anatomical structures form the boundaries or floor of this region?

Which intrinsic muscles of the hand are paralyzed if there is hyperextension of the metacarpophalangeal joint and flexion of the interphalangeal joint?
The patient is presenting with pain around the base of the thumb. Which tendons are likely involved?
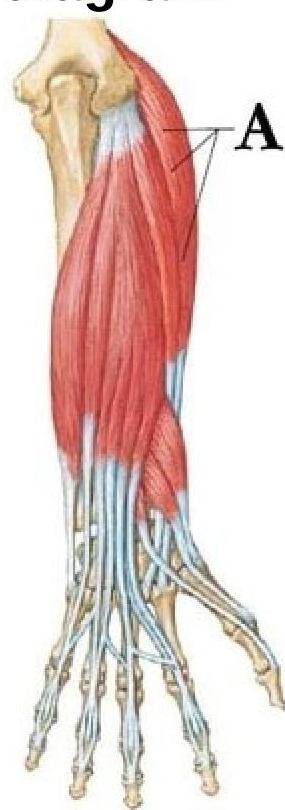
Identify the marked muscle 'A' in the diagram.
Identify the muscles responsible for scapular retraction and elevation. What is their nerve supply?
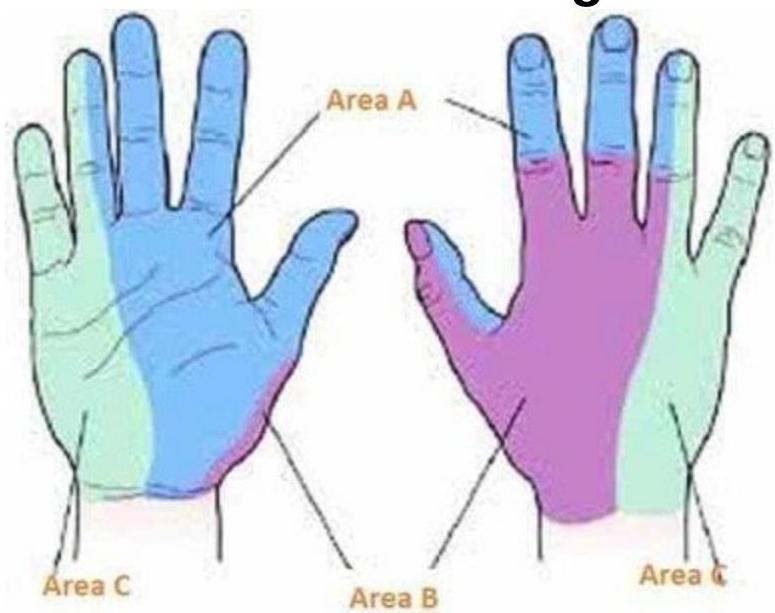
Which nerve supplies the area marked as 'Area B' in the image?
What is the function of the Extensor Carpi Radialis Longus?
Wrist drop is caused by injury to which nerve?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app