
Upper Limb — MCQs

On this page
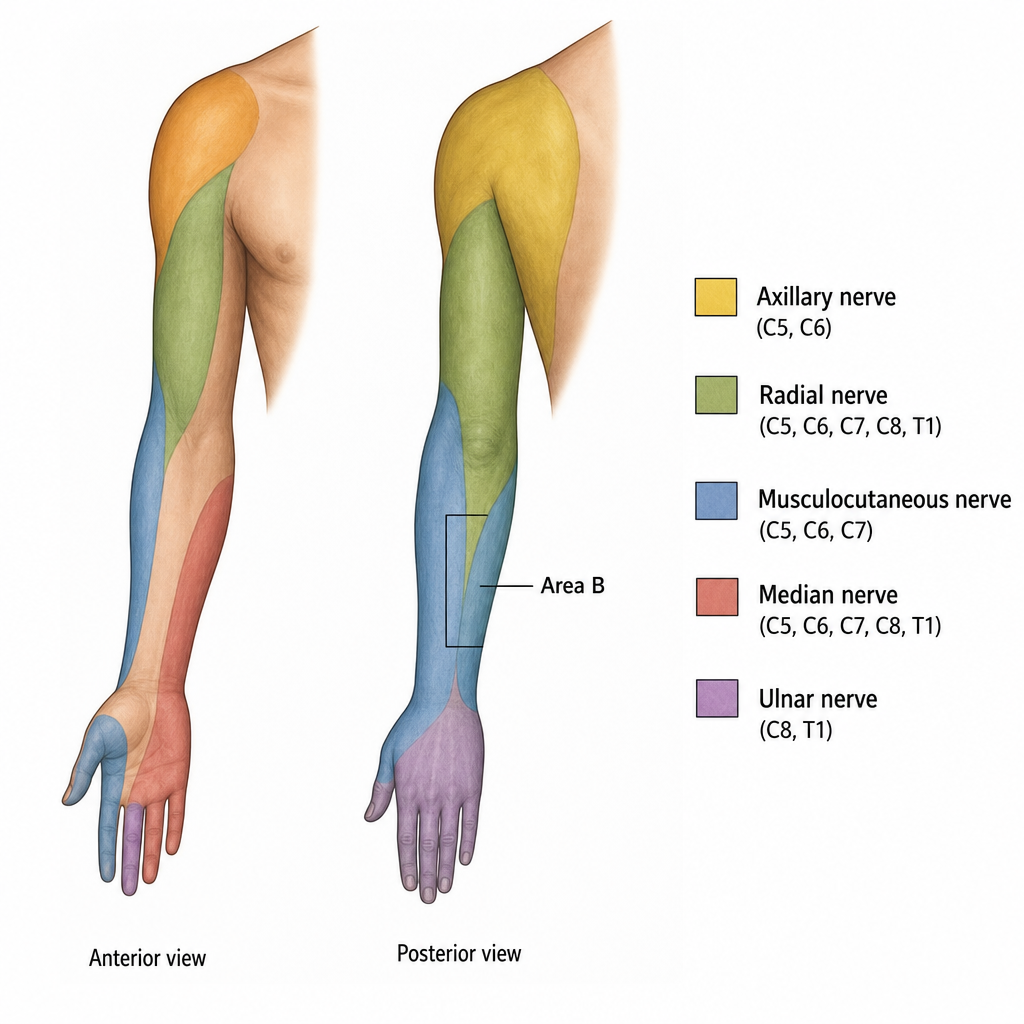
Which nerve supplies the area marked as ‘Area B’ in the image?
Which nerve supplies the rhomboid major and minor muscles?
Identify the marked muscle in the diagram.
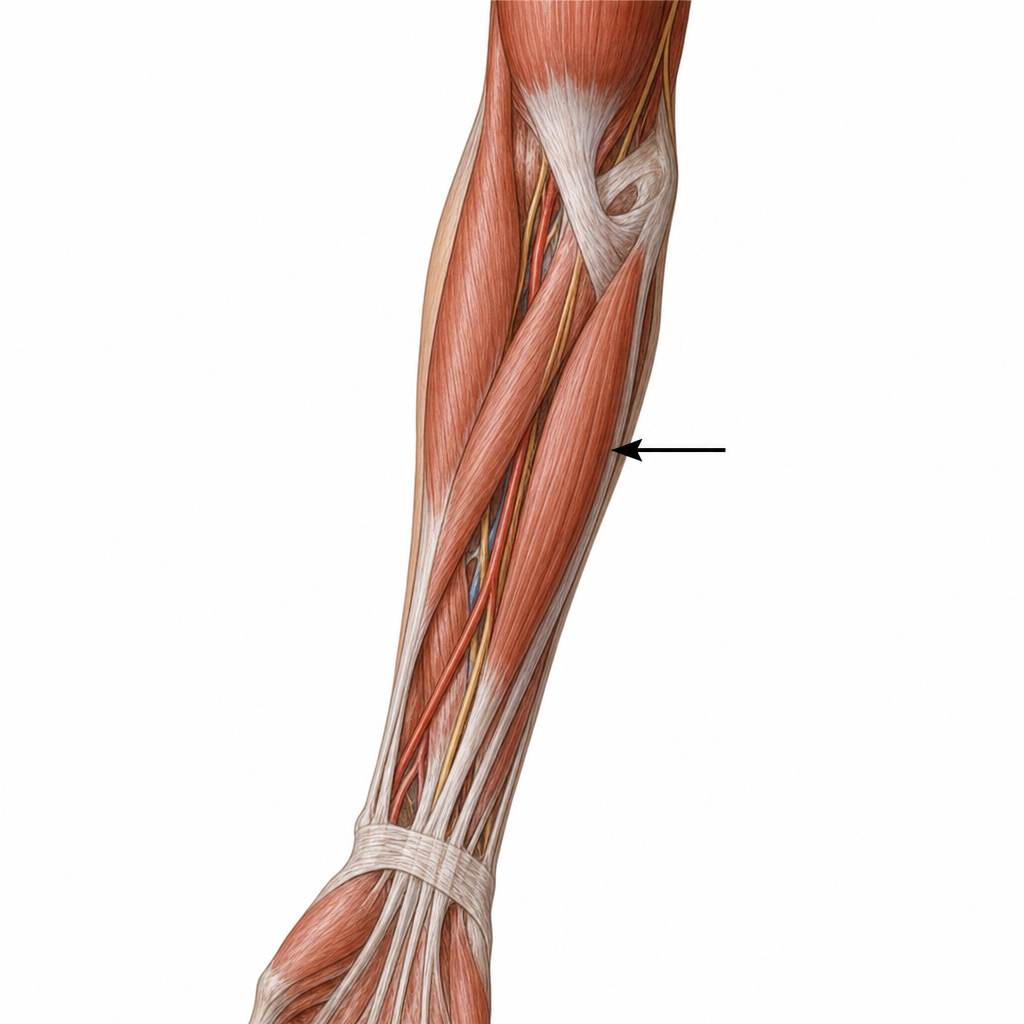
What is the nerve supply of the structure marked in the image?

Identify the anatomical structures visible in the image.

Low radial nerve palsy (just after the spiral groove) does not produce which of the following?
Which of the following arteries contributes MOST to the deep palmar arch?
Pulp of the index finger is supplied by
What type of muscles are medial two lumbricals?
Which muscle acting on the thumb is the only one among the options that has dual nerve supply?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app