
Upper Limb — MCQs

On this page
Which nerve gives sensory supply to the region marked with an arrow?

The test performed below shows testing of which of the following nerve: (Recent NEET Pattern 2016-17)

A patient came with inability to move his 4th and 5th digit and cannot hold pen or paper between his fingers. Which of the following sites shown below is the probable cause of nerve injury to this patient?
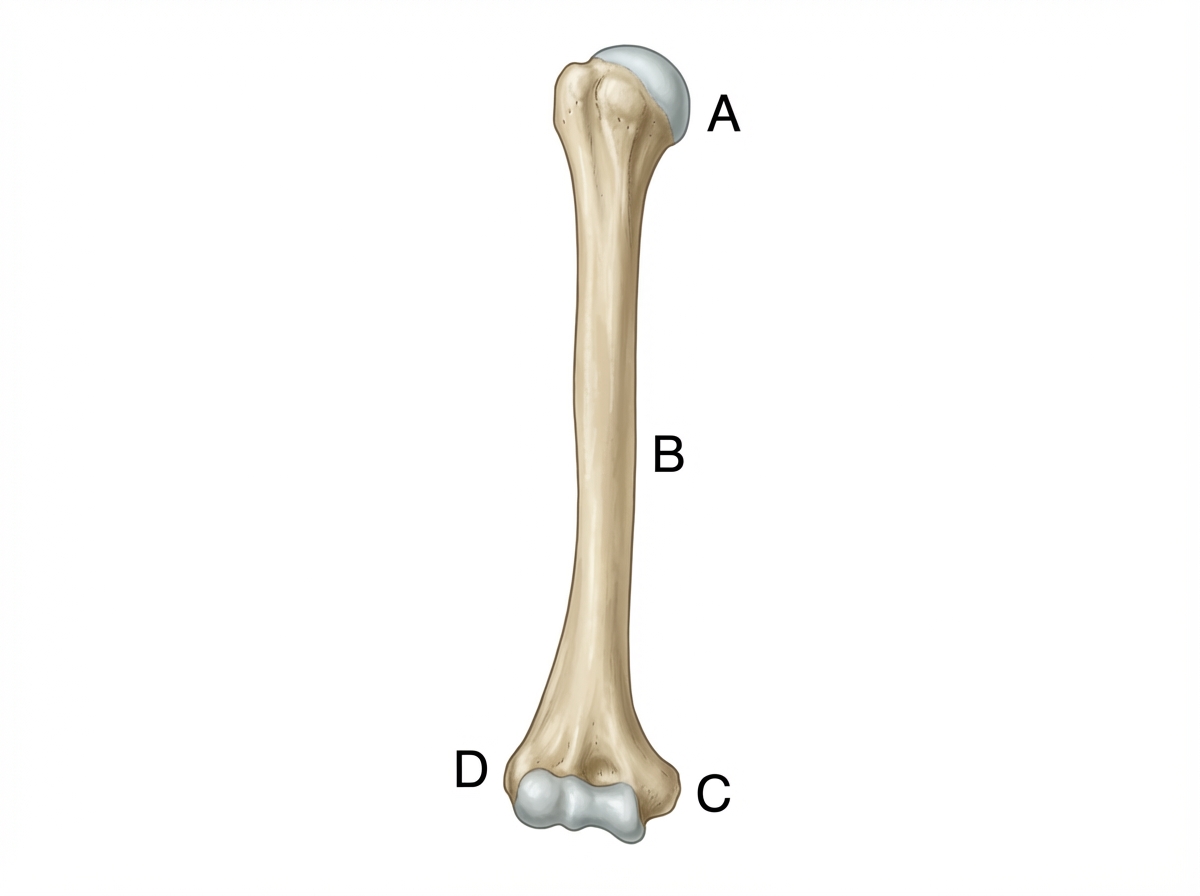
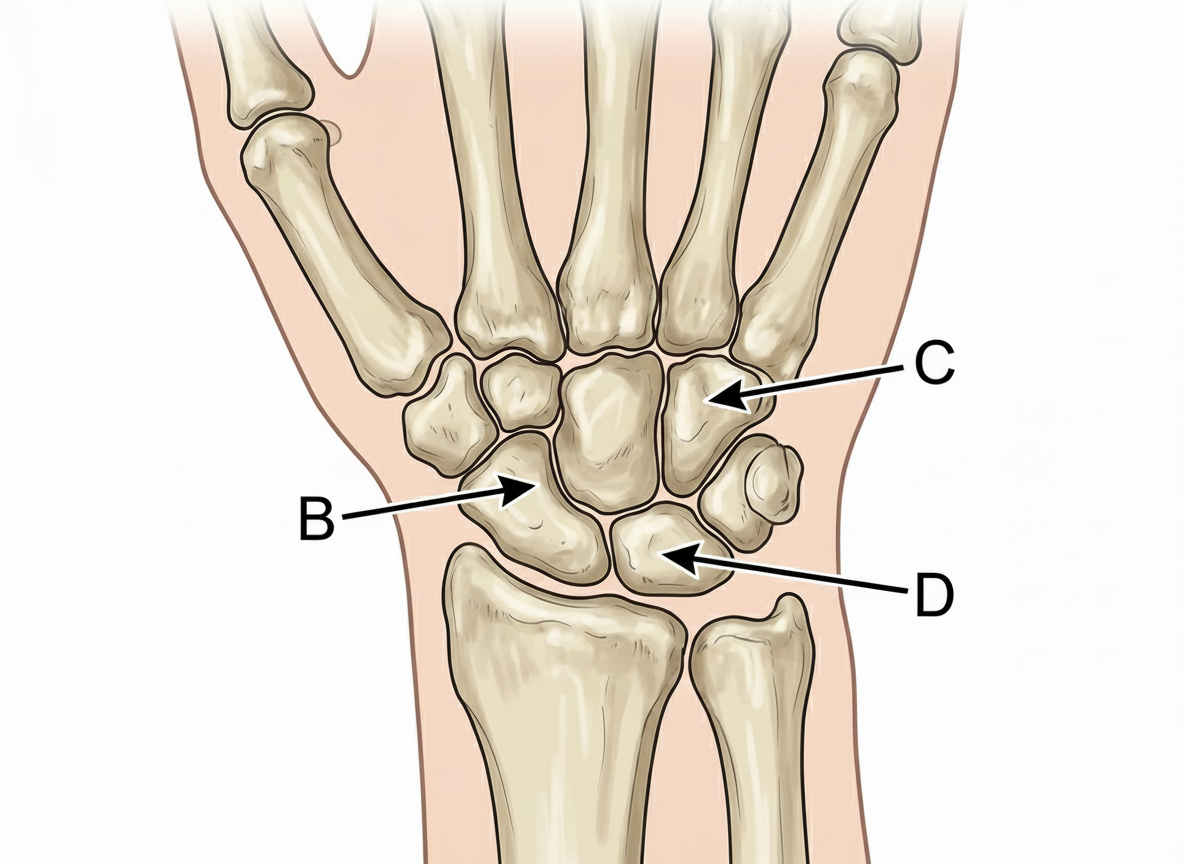
Which of the following bones is the first one to ossify?
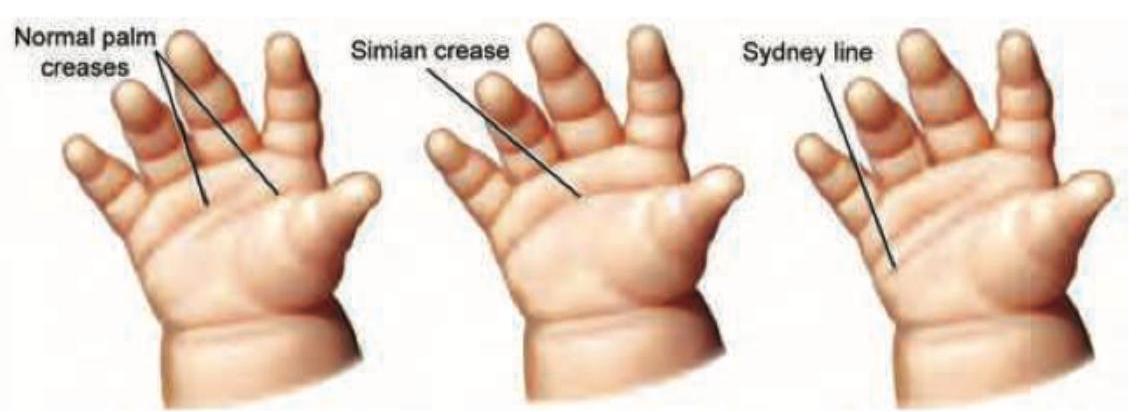
The image displays a hand with a distinct palmar crease pattern where a transverse crease extends from the radial to the ulnar border, in addition to another proximal transverse crease. What is this specific crease pattern called?
Lesion at \qquad level leads to deformity shown in neonate born after prolonged labor?

The inability to flex the index finger is a sign of
A patient presents with loss of sensation on the lateral 3½ fingers and thenar atrophy. Which nerve is most likely involved?
Froment's sign (book test) is used to assess the function of adductor pollicis. Which of the following nerves supplies this muscle?
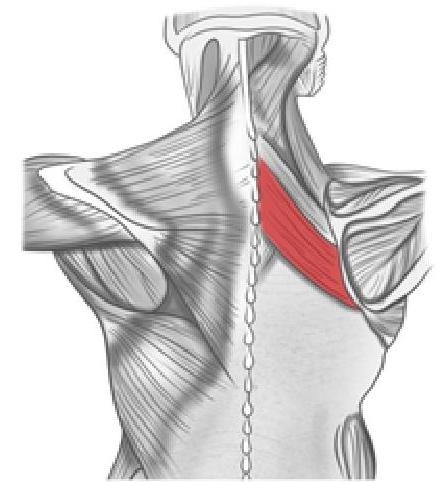
What is the action of the muscle shown in the image below?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app