
Upper Limb — MCQs

On this page
During hyperextension, the long head of triceps gets detached from which site?
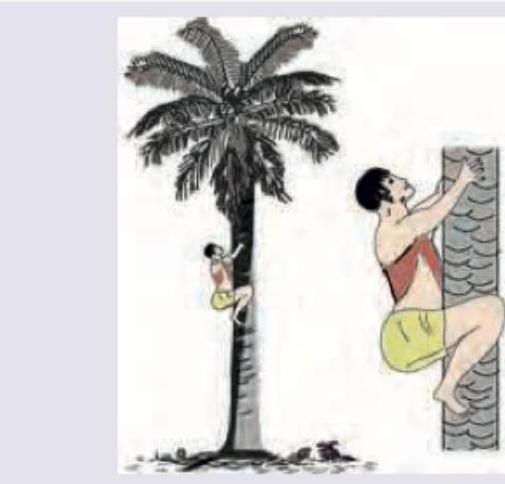
Name the principal muscles traditionally known as climbing muscles being used in climbing a tree as shown in the figure.
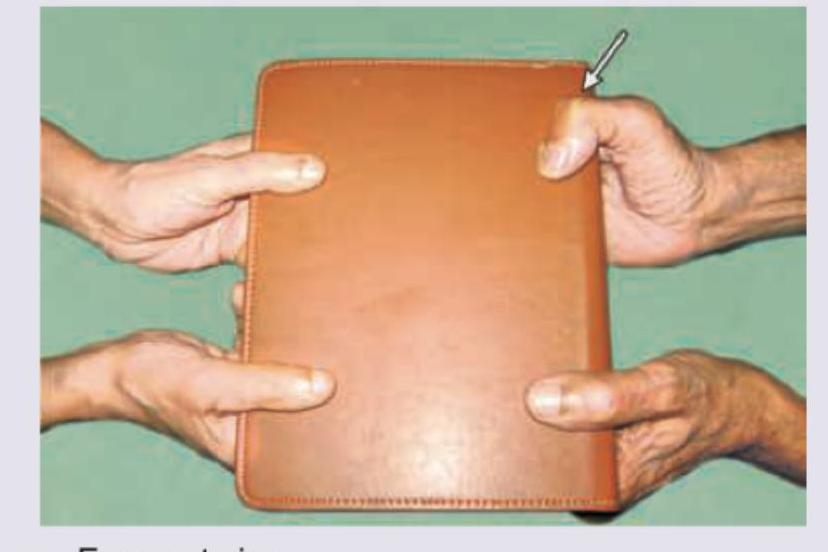
What is incorrect about the test being performed?
Identify the structure marked as X in the specimen of left cubital fossa

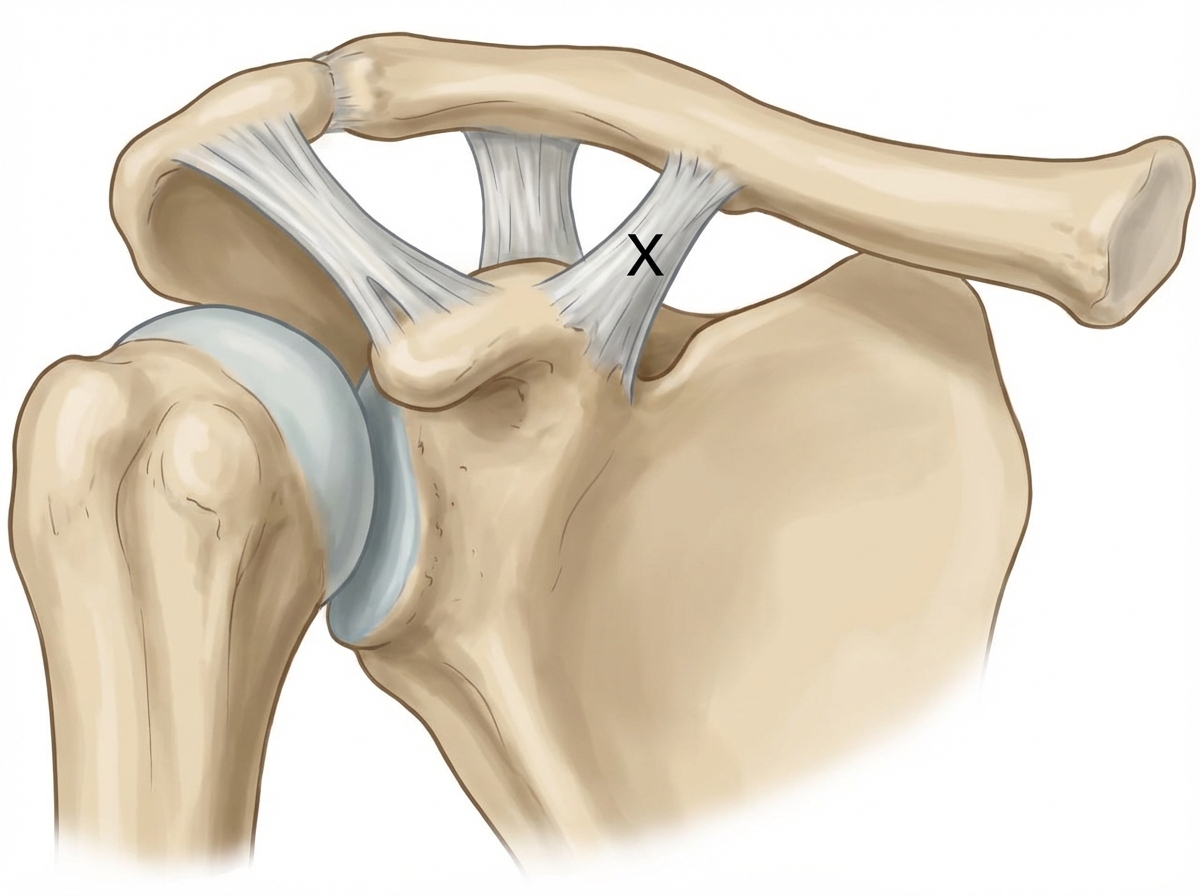
Name the ligament marked as $X$.
All are true about the triangle marked green except:

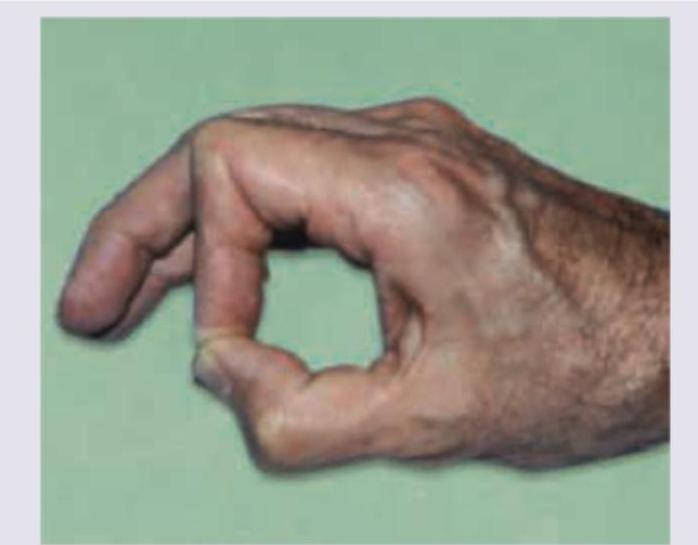
A patient with no sensory loss has isolated inability to flex the interphalangeal joint of the thumb and distal interphalangeal joint of the index finger, producing the abnormal pinch shown. Identify the damaged nerve:
Which nerve supplies the highlighted muscle? (Recent NEET Pattern 2019)

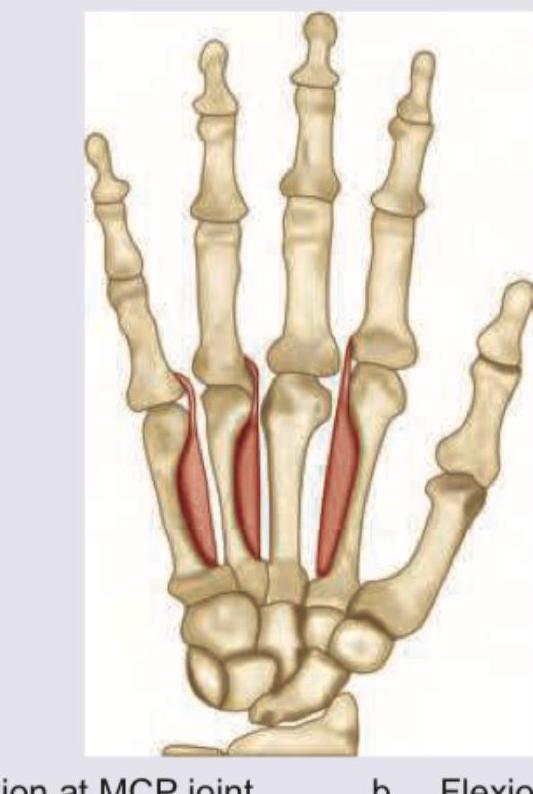
Identify the function of the muscles marked in red:
Name the muscle marked as colour blue in the superficial posterolateral forearm. (Recent NEET Pattern 2019)

Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app