
Upper Limb — MCQs

On this page
A 24-year-old construction worker presents after an injury to his left hand. Physical examination reveals marked flexion of the ring and little fingers. Which of the following additional findings would most likely be found on physical examination?
A 19-year-old male sustained an injury to the C8-T1 spinal nerve roots after a fall. Which of the following nerves, when demonstrating sensory loss in the area it supplies, would confirm the nature of his neurologic injury?
A sixteen-year-old boy receives a superficial cut on the thumb side of his forearm. Which superficial vein is most likely affected?
Which of the following muscles is NOT supplied by the C8 T1 nerve roots?
A 31-year-old patient complains of sensory loss over the anterior and posterior surfaces of the medial third of the hand and the medial one and one-half fingers. The patient is diagnosed with "funny bone" symptoms. Which of the following nerves is injured?
A 23-year-old female sustained an injury to her right index finger while making a bed. She experienced sudden, severe pain over the base of the terminal phalanx, followed by swelling and inability to completely extend the terminal interphalangeal joint. Which one of the following structures within the digit was most likely injured?
Which muscle is attached to the medial border of the scapula?
A 24-year-old medical student was bitten at the base of her thumb by her dog. The wound became infected and the infection spread into the radial bursa. The tendon(s) of which muscle will most likely be affected?
Which of the following muscles is not a hybrid muscle?
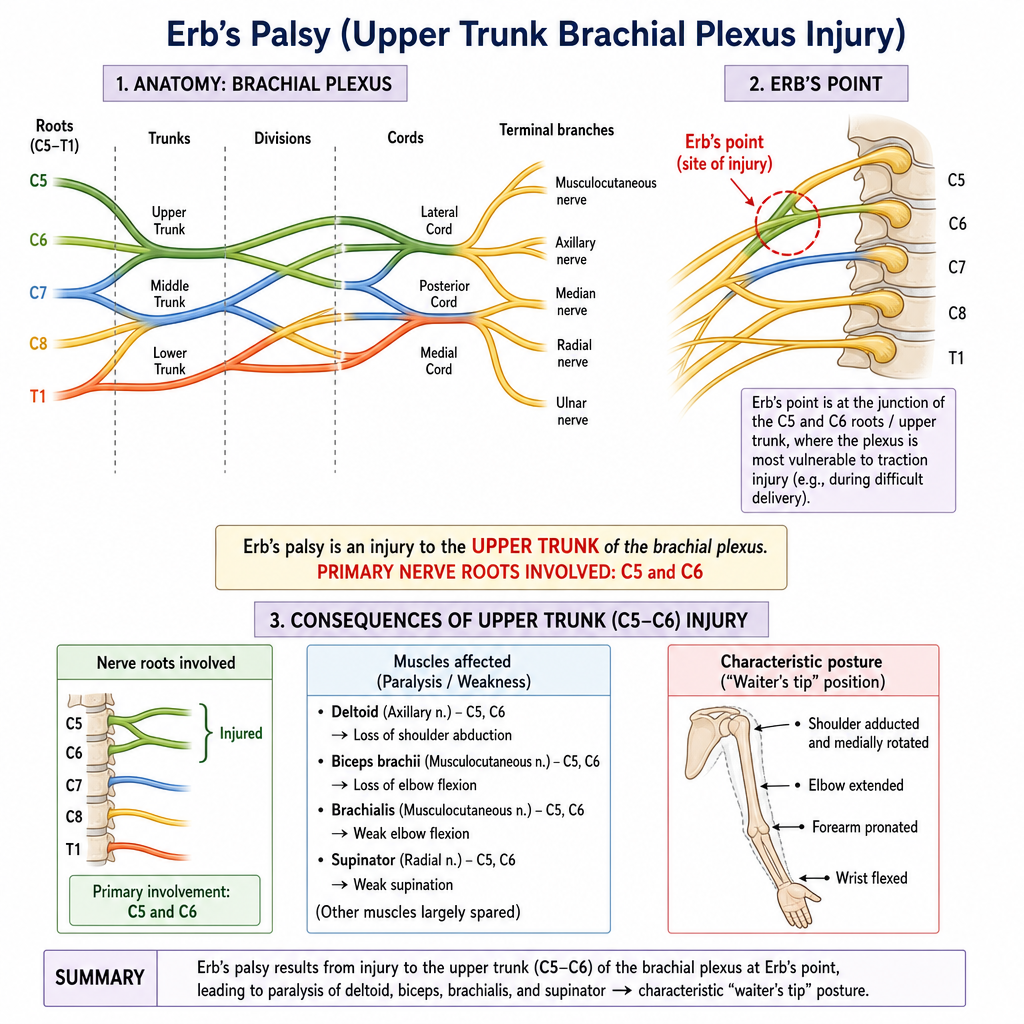
A patient presents with a "waiter's tip" deformity. Based on the unlabeled brachial plexus diagram , which of the following nerve roots are primarily involved in this type of brachial plexus injury, often termed Erb's palsy, as indicated by Erb's point?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app