
Upper Limb — MCQs

On this page
Which of the following structures passes through the triangular interval of the arm?
Boundaries of the anatomical snuff box are all except?
A patient presents with loss of sensation in the lateral three and a half fingers. Which of the following will be an additional finding in this patient?
The superficial palmar arch is related to which anatomical landmark?
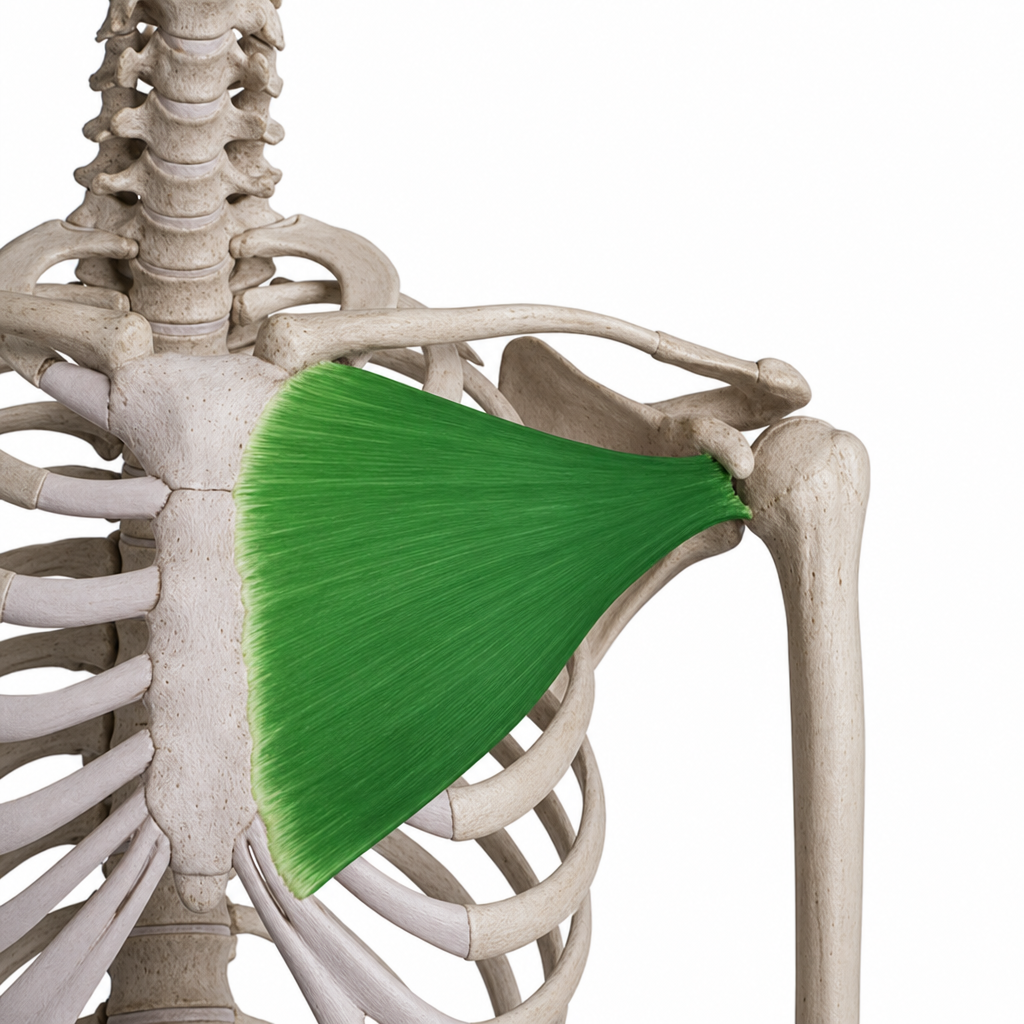
What is the primary action of the highlighted muscle?
Which nerve is injured in a fracture of the medial epicondyle of the humerus?
Which of the following structures is located within the bicipital groove?
Which structure lies lateral to the distal radial tubercle?
Which of the following statements regarding the adductor pollicis muscle is false?
Which of the following fingers has two dorsal interossei muscles?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app