
Upper Limb — MCQs

On this page
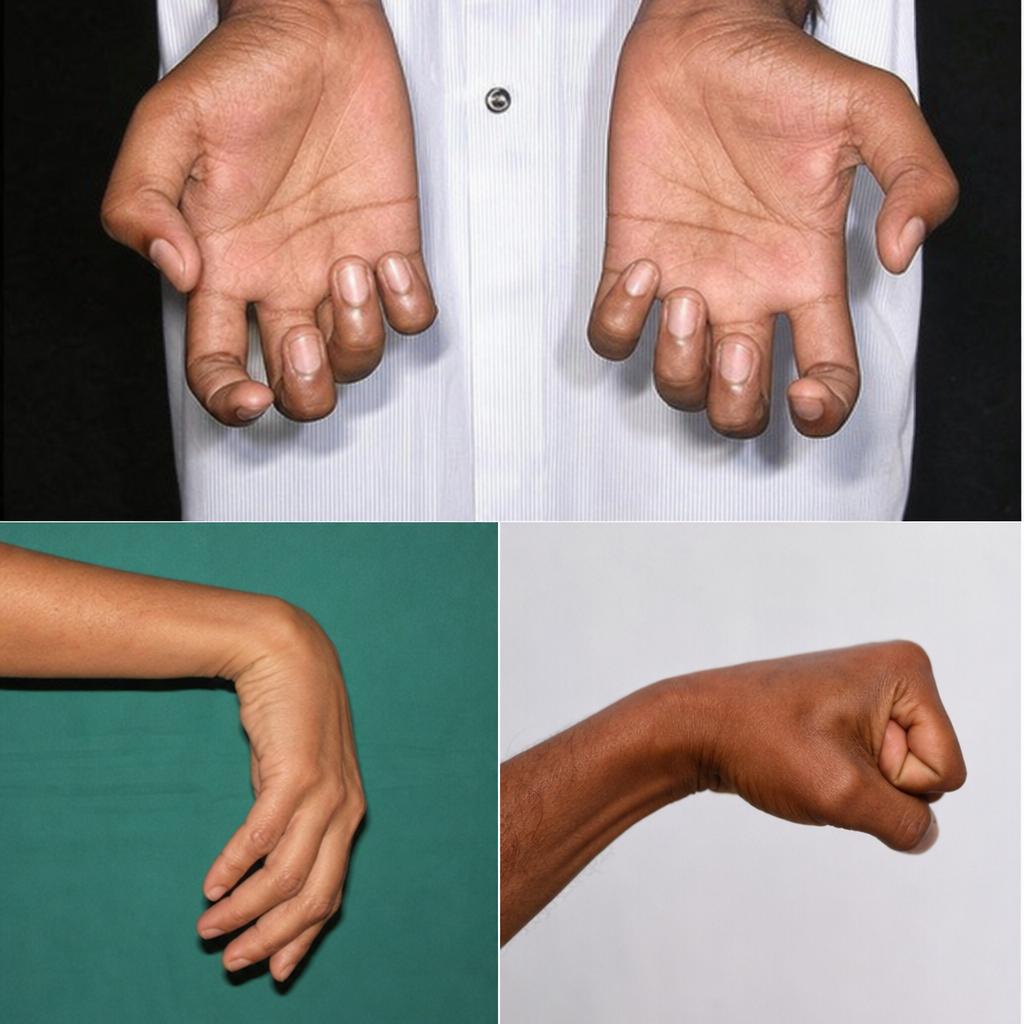
A 35-year-old man presents after a traumatic injury to his arm. On examination, he has clawing of all four fingers, wasting of both the thenar and hypothenar eminences, loss of all intrinsic hand muscle function, and reduced sensation over the medial forearm and hand including the little finger and medial half of the ring finger. Reflexes are intact at the elbow. Which of the following best explains this hand deformity?
Which of the following forms the anterior wall of the axilla?
Lymphatics from the upper limb drain into which group of axillary nodes?
Following a radical mastectomy, there is injury to the long thoracic nerve. How can the integrity of this nerve be tested at the bedside?
Deformity associated with ulnar nerve injury is:
Which muscle causes flexion at the elbow joint when the forearm is semi-pronated?
Intracapsular articular disc is present in which joint?
All the muscles are used to abduct the shoulder except?
Which muscle is typically spared in a lateral epicondyle fracture?
Which of the following is least likely to be involved in a collateral anastomosis which bypasses an obstruction of the first part of the axillary artery?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app