
Upper Limb — MCQs

On this page
Axillary abscess is safely drained by which approach?
Which carpal bone articulates with the radius?
Which of the following arteries is present in the anatomical snuff box?
Which muscle arises from the supraglenoid tubercle?
Which muscle is inserted into the floor of the intertubercular sulcus of the humerus?
A rock climber falls on their shoulder, resulting in a chipping off of the lesser tubercle of the humerus. Which of the following structures would most likely have structural and functional damage?
A patient has a tiny (0.2 cm), but exquisitely painful tumor under the nail of her index finger. Prior to surgery to remove it, local anesthetic block to a branch of which of the following nerves would be most likely to achieve adequate anesthesia?
Which nerve passes through the spiral groove of the humerus?
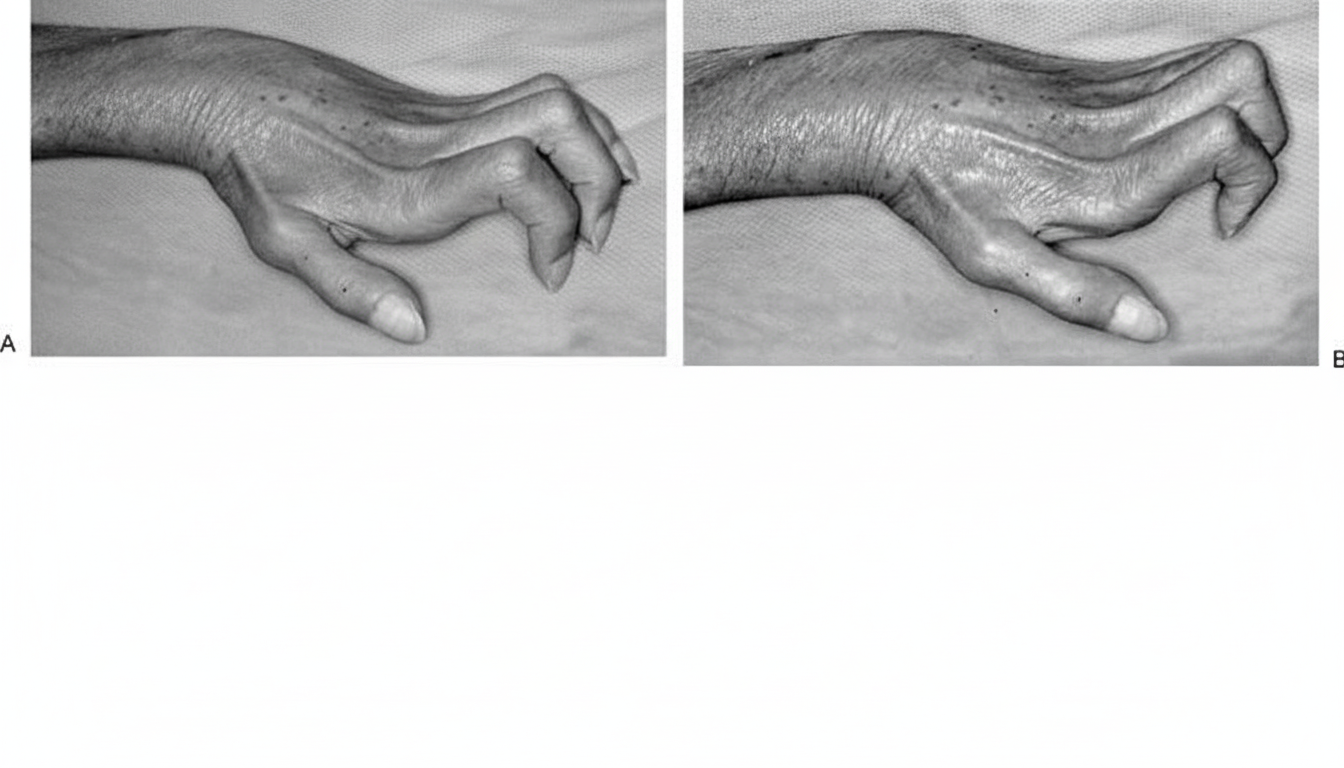
What is the nerve injury that causes a "claw hand" deformity as shown in the image?
Which among the following muscles receives dual nerve supply?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app