
Upper Limb — MCQs

On this page
The middle radio-ulnar joint is a type of what?
Which of the following statements about the ulnar nerve is correct?
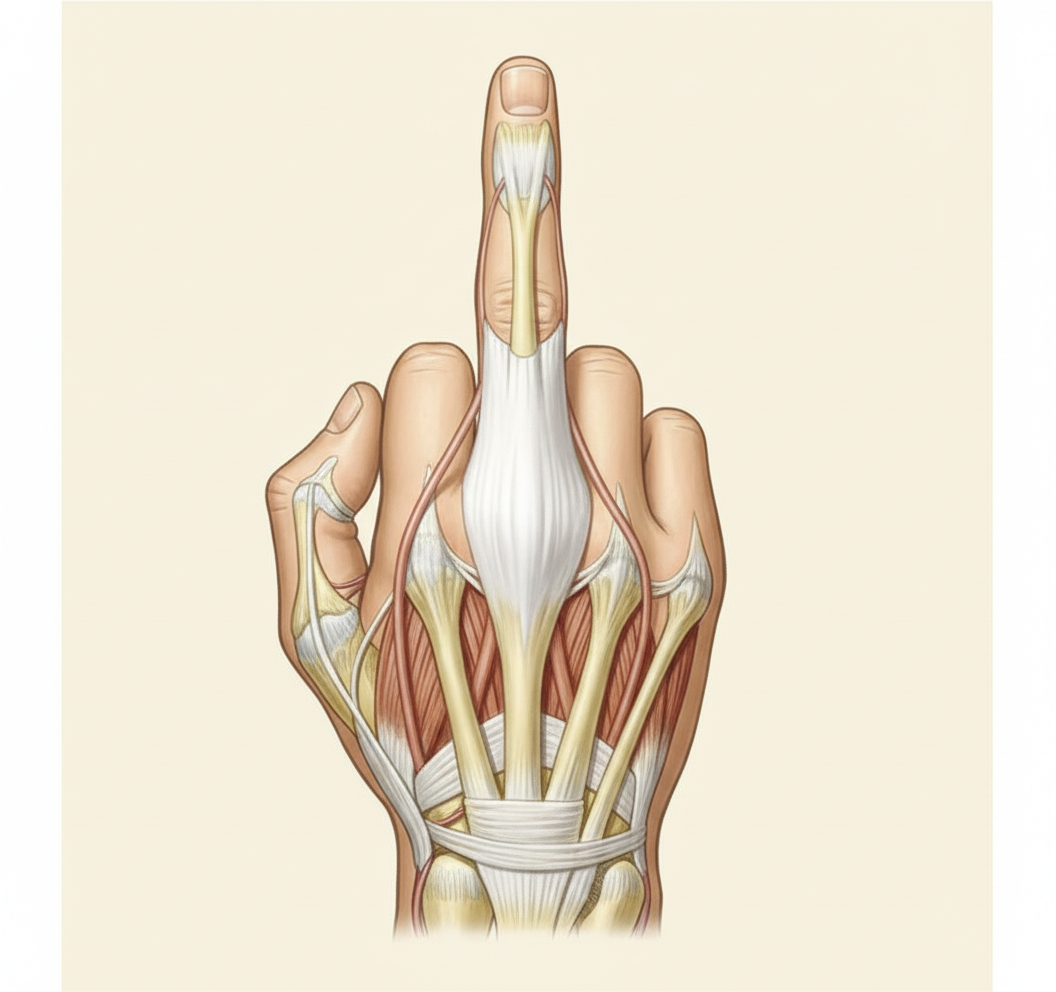
Which of the following muscles do not contribute to the marked tendon?
Which of the following is a synovial joint of the condylar variety?
The first lumbrical canal communicates with which of the following spaces?
All of the following bony structures form the floor of the anatomical snuff box, EXCEPT?
The pronator quadratus muscle shares its innervation with which of the following muscles?
A day after a left-sided lumpectomy and axillary dissection, a 63-year-old woman is experiencing difficulty elevating her left arm. She cannot fully raise her upper arm from the side of her body. The median border and inferior angle of the left scapula become unusually prominent when she pushes against the wall with both hands. The innervation of which of the following muscles was most likely injured during the surgery?
What are the clinical manifestations of Klumpke's paralysis?
The short head of the biceps brachii muscle is attached to which anatomical structure?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app