
Upper Limb — MCQs

On this page
Which nerve passes through the medial epicondyle?
Allen's test is used for detecting the integrity of which of the following?
Which nerve originates from the trunk of the brachial plexus?
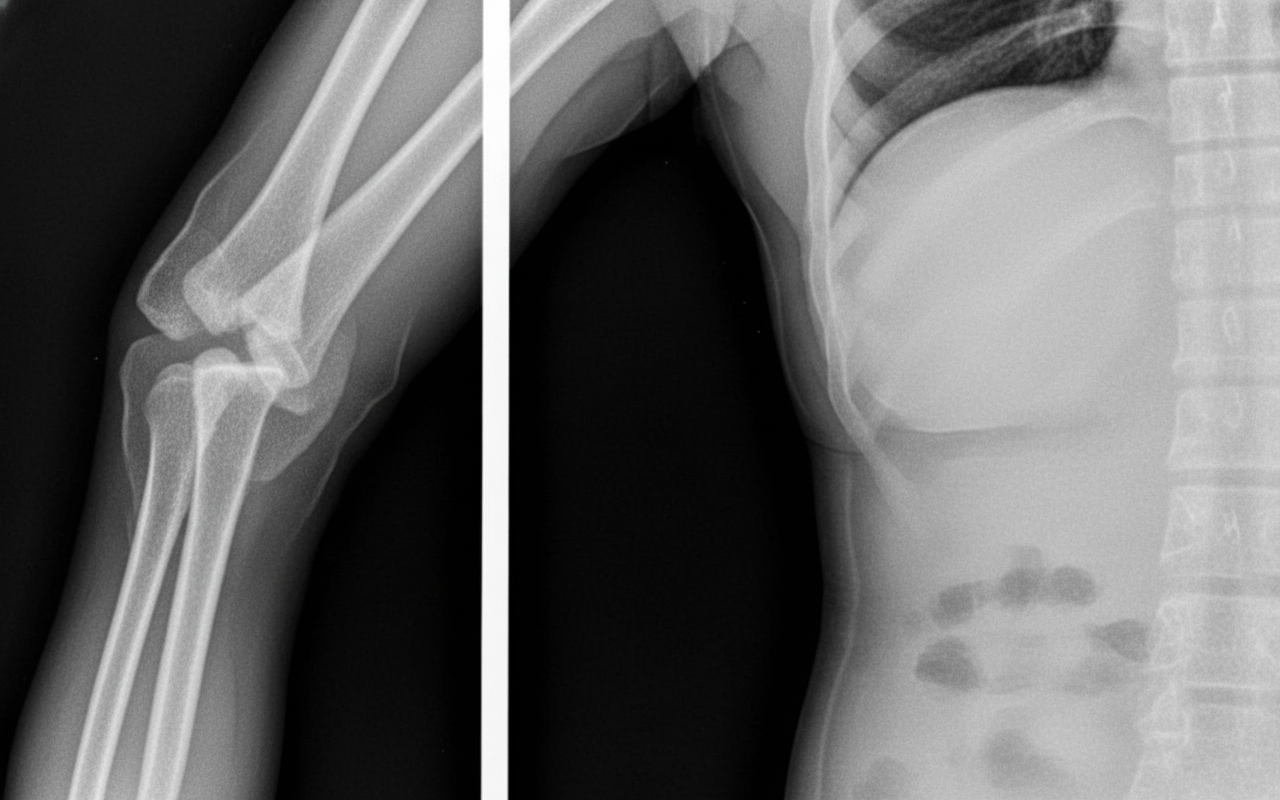
A 50-year-old male patient presented with an elbow dislocation as shown in the x-ray. On examination, there was paralysis of most of the intrinsic muscles of the hand and loss of sensation from the medial 1.5 palmar surface of fingers. Which of the following nerves arise from the same cord as the injured nerve, except?
You order a wrist X-RAY for a 2-month-old child. Which carpal bone are you expecting to be present?
Which artery is NOT involved in the vascular anastomosis around the acromion?
Which of the following statements about the first metacarpal is false?
A 45-year-old male presents with injuries to his left elbow after a fall. Radiographic and MRI examinations reveal a fracture of the medial epicondyle and a torn ulnar nerve. Which of the following muscles would be most likely to be paralyzed?
Which tendon is present in the third extensor compartment of the wrist?
What is the nerve supply of the pronator teres muscle?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app