
Upper Limb — MCQs

On this page
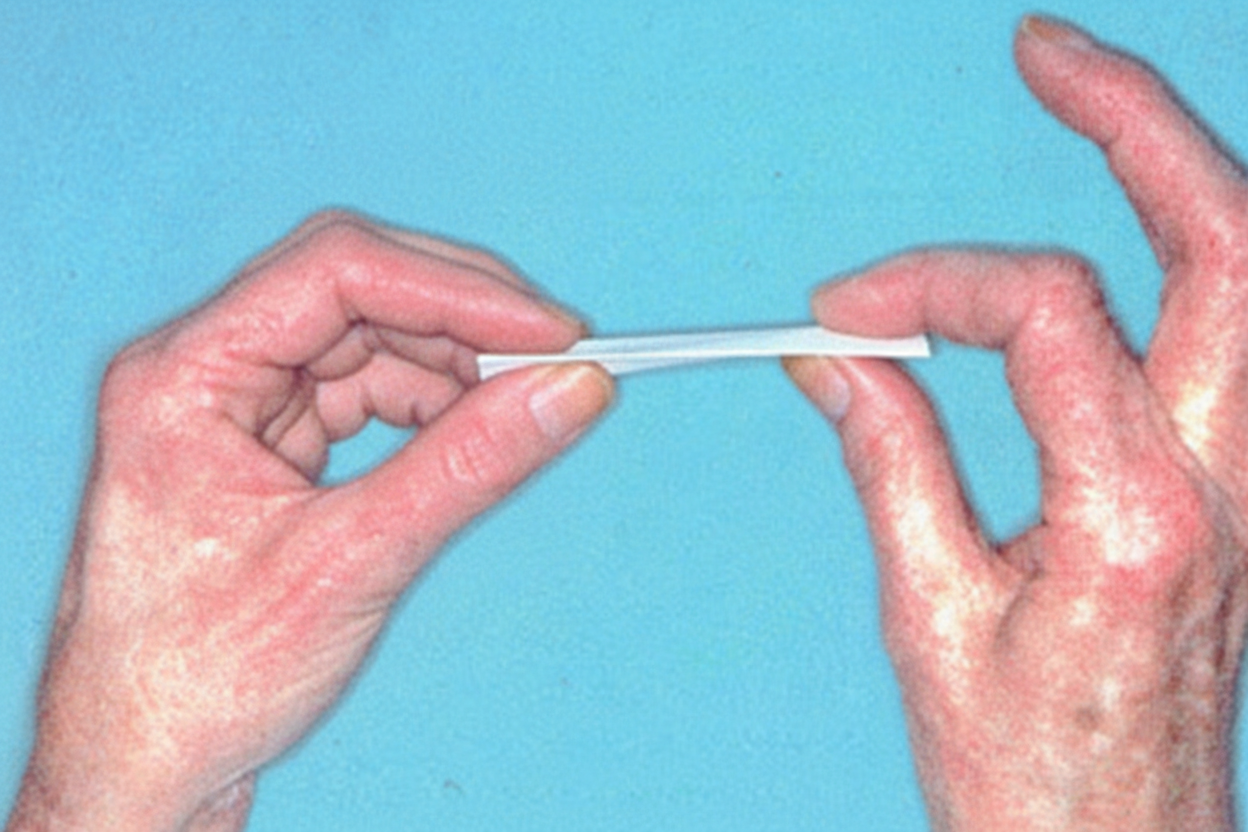
For which of the following nerve palsies is the below test detected?
A patient presents with a deep stab wound in the middle of the forearm, resulting in impaired movement of the thumb. Examination suggests a lesion of the anterior interosseous nerve. Which of the following muscles is paralyzed?
Which of the following muscles is spared when the radial nerve is injured in the radial groove?
Regarding the axilla, which of the following statements is accurate?
Which dermatome corresponds to the middle finger?
Damage to the C7 nerve root causes weakness of which of the following movements?
Which of the following movements of the thumb is lost in ulnar nerve injury?
The musculocutaneous nerve is a branch of which part of the brachial plexus?
Which maneuver is used to test for integrity of the long thoracic nerve?
The radial styloid process gives attachment to which of the following muscles?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app