
Upper Limb — MCQs

On this page
Fracture of the surgical neck of the humerus leads to loss of abduction movement of the corresponding shoulder joint due to injury of which nerve?
Intramuscular injections are typically administered in which part of the deltoid muscle?
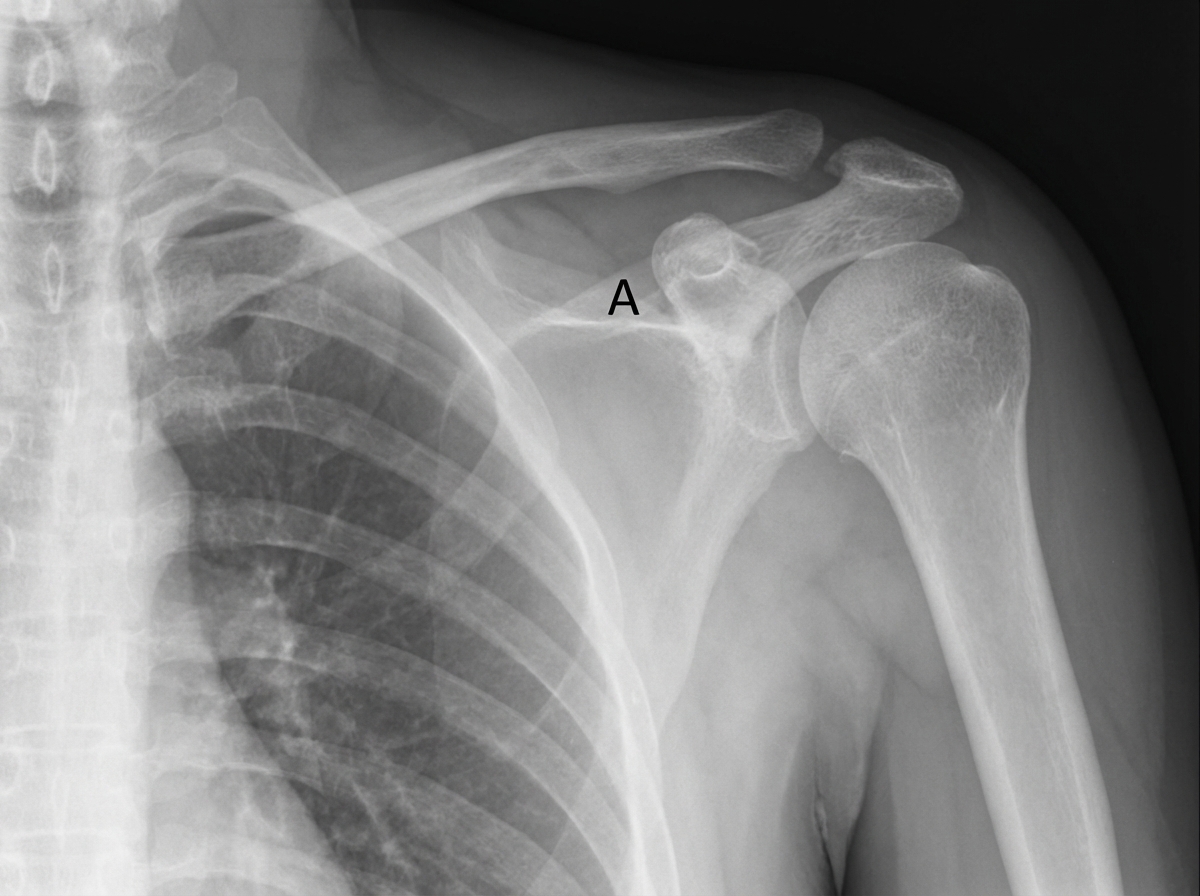
An 11-year-old boy falls down the stairs. A physician examines a radiograph of the boy's shoulder region. If the structure indicated by the letter A is calcified, which of the following muscles is most likely paralyzed?
What is the action of the anterior fibers of the deltoid muscle?
A 27-year-old patient presents with an inability to draw the scapula forward and downward because of paralysis of the pectoralis minor. Which of the following would most likely be a cause of his condition?
Which of the following statements about the supraspinatus is FALSE?
The cords of the brachial plexus are named relative to the axillary artery. Which muscle lies behind the axillary artery in relation to these cords?
The anterior interosseous nerve is a branch of which of the following?
A 41-year-old male presents with weakness of the flexor pollicis longus and flexor digitorum profundus of the index finger. Which nerve is most likely involved?
A patient presents with inability to extend the wrist following an accident. The patient reports no sensory loss. At what anatomical location is the affected nerve most likely injured?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app