
Upper Limb — MCQs

On this page
A 32-year-old man is diagnosed with a herniated disc impinging the spinal nerve that exits inferior to the C6 vertebra. Pain from the impinged nerve would most likely radiate to which cutaneous region?
What is the characteristic of Poland Syndrome?
Boundaries of the upper triangular space include all except?
All of the following are affected in low radial nerve palsy except?
Which structure passes deep to the flexor retinaculum at the wrist?
A patient is diagnosed to have anterior interosseous nerve syndrome. Which of the following muscles is not affected in this syndrome?
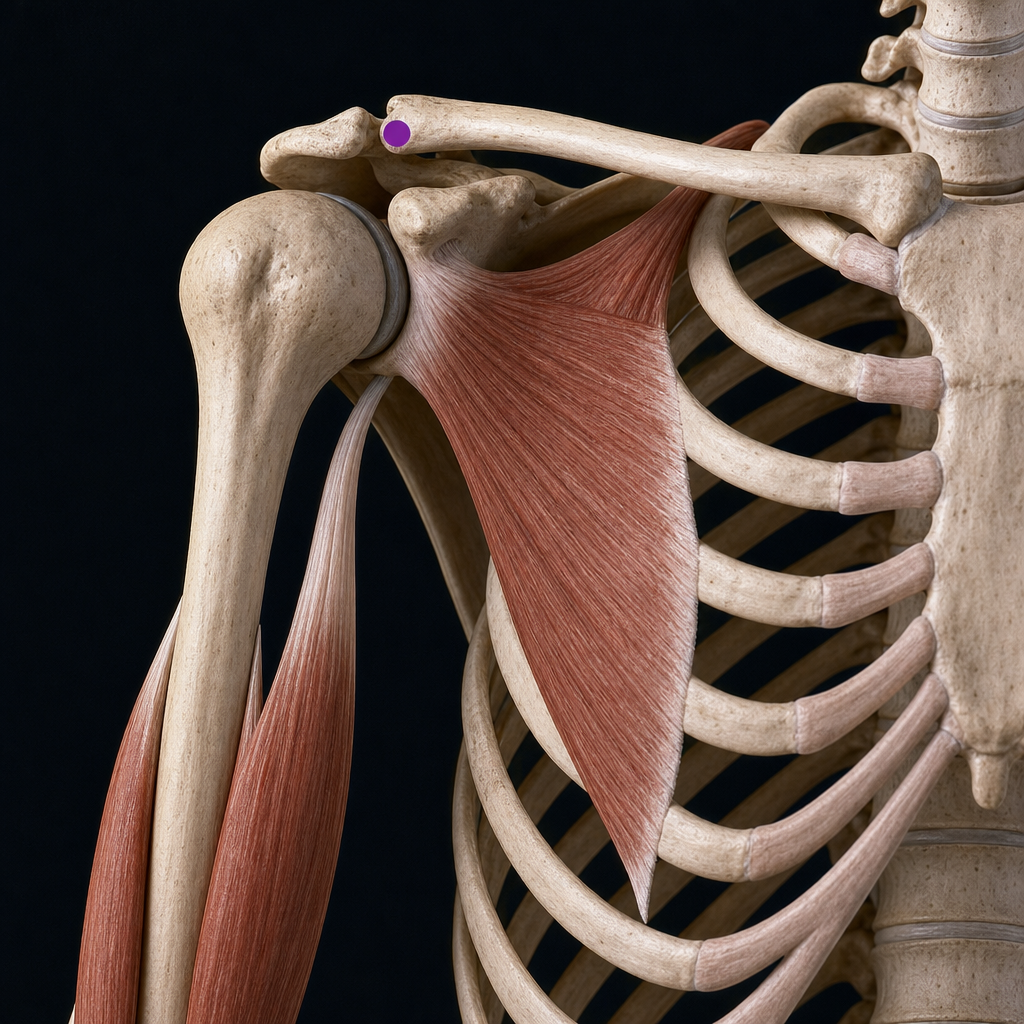
Which of the following muscles has an attachment on the marked part?
A 48-year-old female court stenographer is admitted to the orthopedic clinic with symptoms of carpal tunnel syndrome, with which she has suffered for almost a year. Which muscles most typically become weakened in this condition?
Which of the following arteries is a branch of the first part of the axillary artery?
While carrying a heavy suitcase, the downward dislocation of the glenohumeral joint is resisted by which of the following muscles EXCEPT?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app