
Upper Limb — MCQs

On this page
Extension at the MCP joint is primarily achieved by which of the following muscles?
Which muscle produces supination when the elbow is flexed?
All of the following muscles elevate the scapula, EXCEPT:
During a strenuous game of tennis, a 55-year-old woman complained of severe shoulder pain that forced her to quit the game. During physical examination, it was found that she could not initiate abduction of her arm, but if her arm was passively elevated to 45 degrees from the vertical (at her side) position, she had no trouble fully abducting it. Injury to which muscle was responsible?
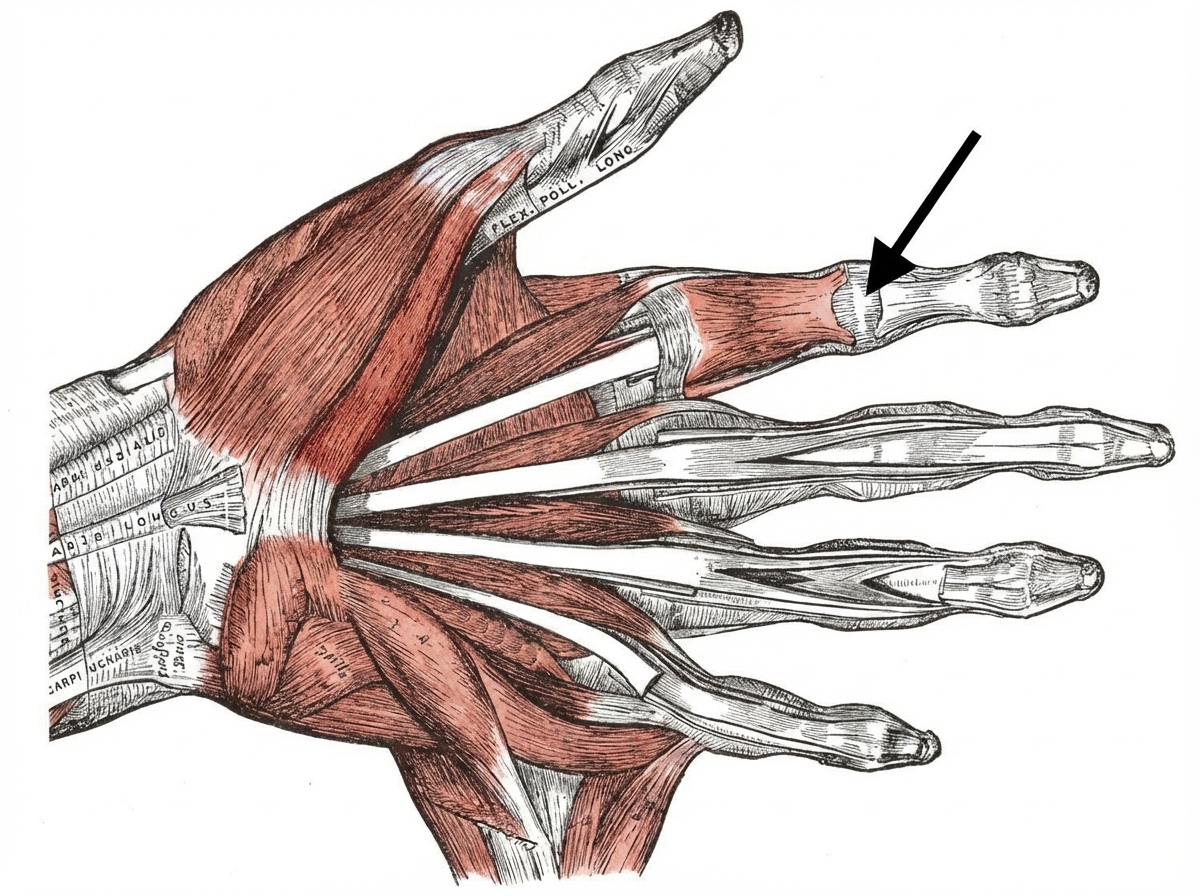
A patient presents with inability to flex her hand at the joint indicated by a black arrow. Which of the following muscles appears to be paralyzed upon further examination of her finger?
Which of the following muscles of the scapula, functioning as retractors, is the exception?
Which of the following muscles is NOT supplied by the radial nerve below the spiral groove?
Which of the following statements about radial nerve palsy is NOT true?
The dorsal scapular nerve supplies all of the following muscles except?
Regarding the anatomical snuffbox, which of the following statements is true?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app