
Upper Limb — MCQs

On this page
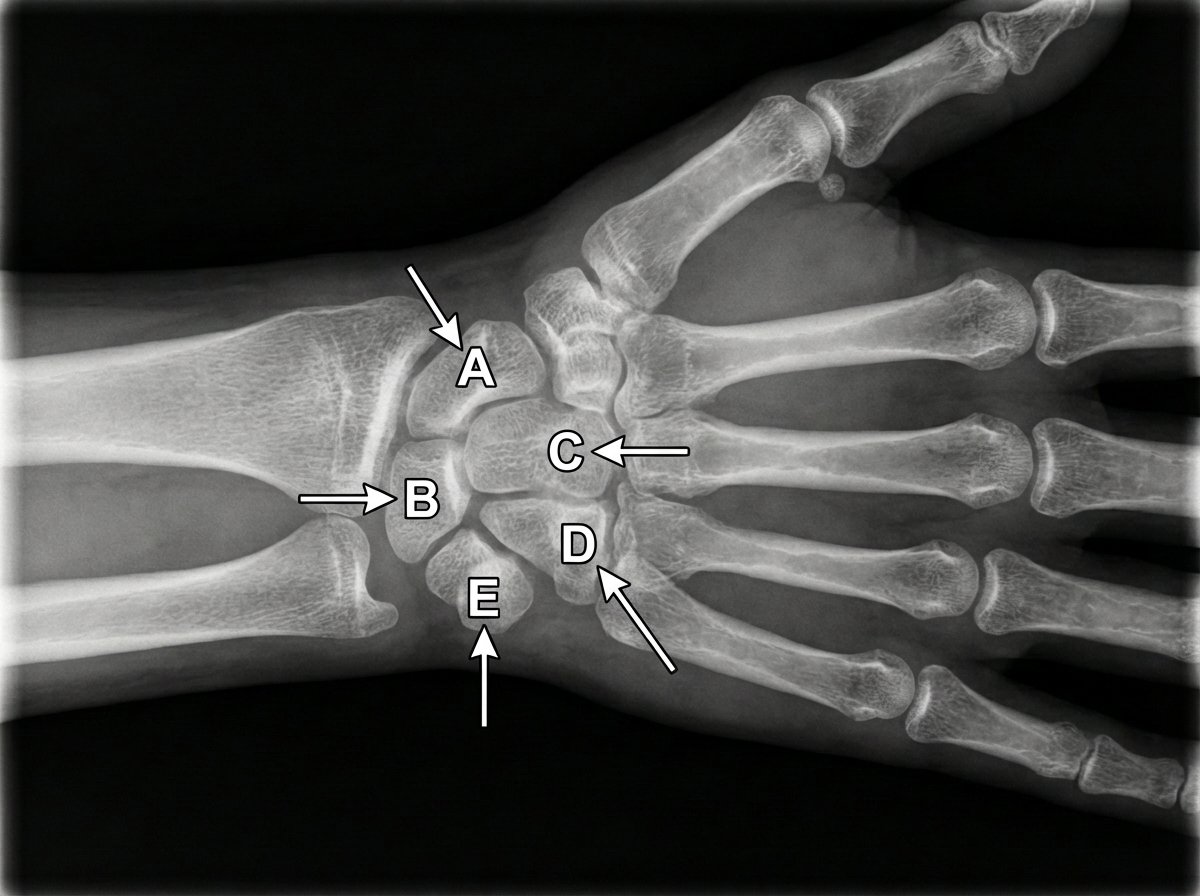
An X-ray of the wrist and hand is shown below. If there is an avulsion injury disrupting the flexor carpi ulnaris insertion at structure E, which of the following muscle weaknesses does it cause?
What is the nerve supply of the opponens pollicis muscle?
Which of the following statements about the scapula is false?
Which muscle of the hand is NOT supplied by the median nerve?
Following anterior dislocation of the shoulder, a patient develops weakness of flexion at the elbow and lack of sensation over the lateral aspect of the forearm. Which nerve is injured?
Which nerve is involved in this presentation?

Which of the following bones has an epiphysis at its base?
Which of the following is NOT a part of the proximal row of carpal bones?
A 37-year-old man suffers a traumatic injury to the axilla that damages the thoracodorsal nerve. Which of the following movements of the arm or scapula could be affected in this patient?
Axillary artery occlusion affects all EXCEPT:
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app