
Upper Limb — MCQs

On this page
A 24-year-old medical student received a booster dose of hepatitis B vaccination, following which she developed weakness in abduction and lateral rotation of the arm. The lesion is most likely to be in which of the following nerves?
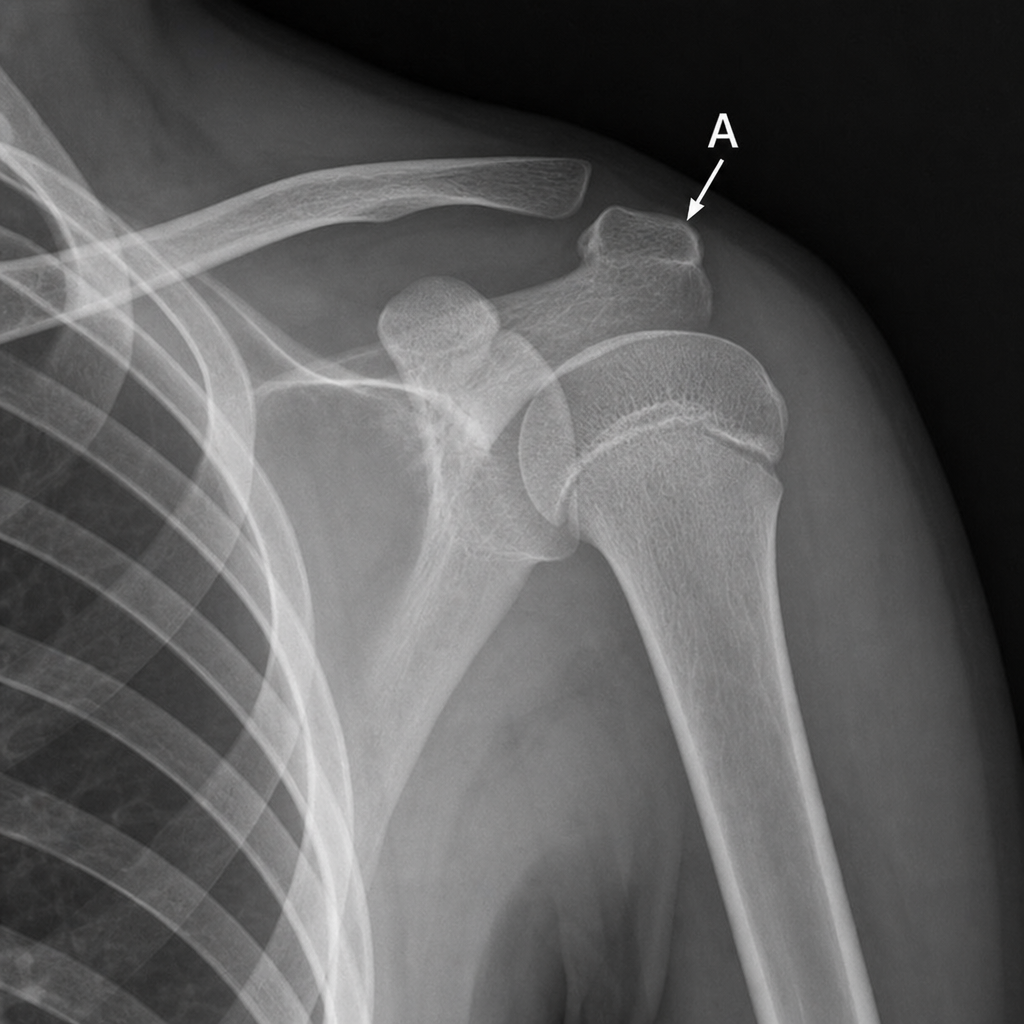
The arrow indicates the base of the coracoid process. MRI demonstrates a ganglion cyst compressing the nerve as it passes through the suprascapular notch, immediately medial to this landmark. Which muscle is most likely to show denervation?
A 50-year-old electrician reports pain in his left upper extremity and tingling and numbness in the 4th and 5th digits of his left hand. There is mild swelling of the left hand. The patient reports most of his pain and numbness occurs when he is doing electrical work with his arms overhead. X-ray reveals the presence of a cervical rib. Which of the following structures is most likely being compressed?
A 43-year-old man presents with a whiplash injury after his car was struck from behind. An MRI reveals cervical disk herniation. Physical examination shows loss of elbow extension, absence of the triceps reflex, and loss of extension of the metacarpophalangeal joints on the ipsilateral side. Which spinal nerve is most likely affected?
All of the following are associated with pronator syndrome, except?
Which structure is intracapsular but extrasynovial?
A knife wound to the neck damages the posterior cord of the brachial plexus. Which of the following muscles would be most likely to be paralyzed?
All of the following bones form the proximal row of carpal bones except?
Which nerve is involved in Guyon's canal syndrome?
The palmar interossei are supplied by which nerve branch?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app