
Upper Limb — MCQs

On this page
Which nerve arises from a root of the brachial plexus?
The neurovascular bundle in the axilla is surrounded by a sheath derived from which structure?
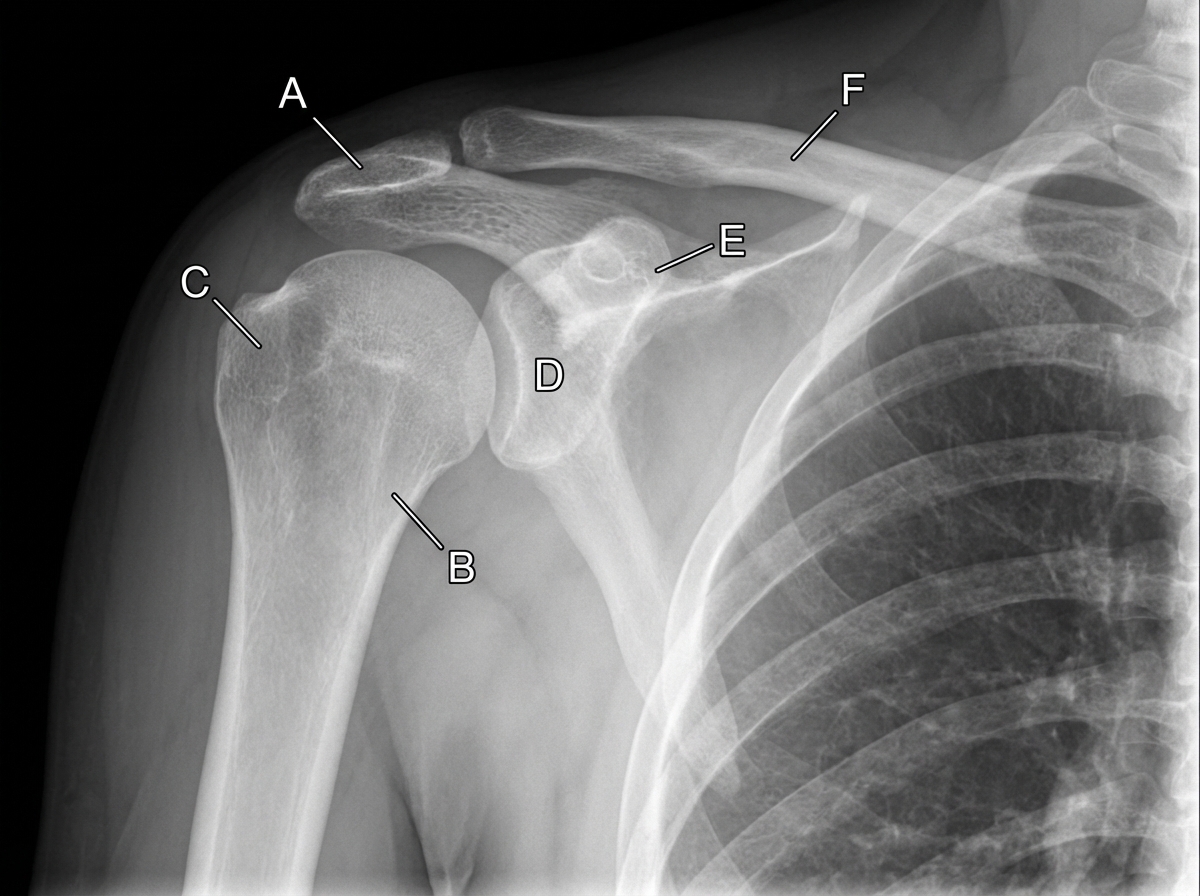
A 35-year-old man falls down the stairs. A physician examines a radiograph of the man's shoulder region. If the structure indicated by the letter B is fractured, which of the following structures is most likely injured?
The forcible separation of the head of the radius from the capitulum of the humerus is mainly prevented by which structure?
Which border of the scapula is not palpable?
A female presented with loss of extension of the little and ring finger, hypothenar atrophy, and metacarpophalangeal joint hyperextension. Which nerve is injured?
The carpometacarpal joint of the thumb is a type of joint?
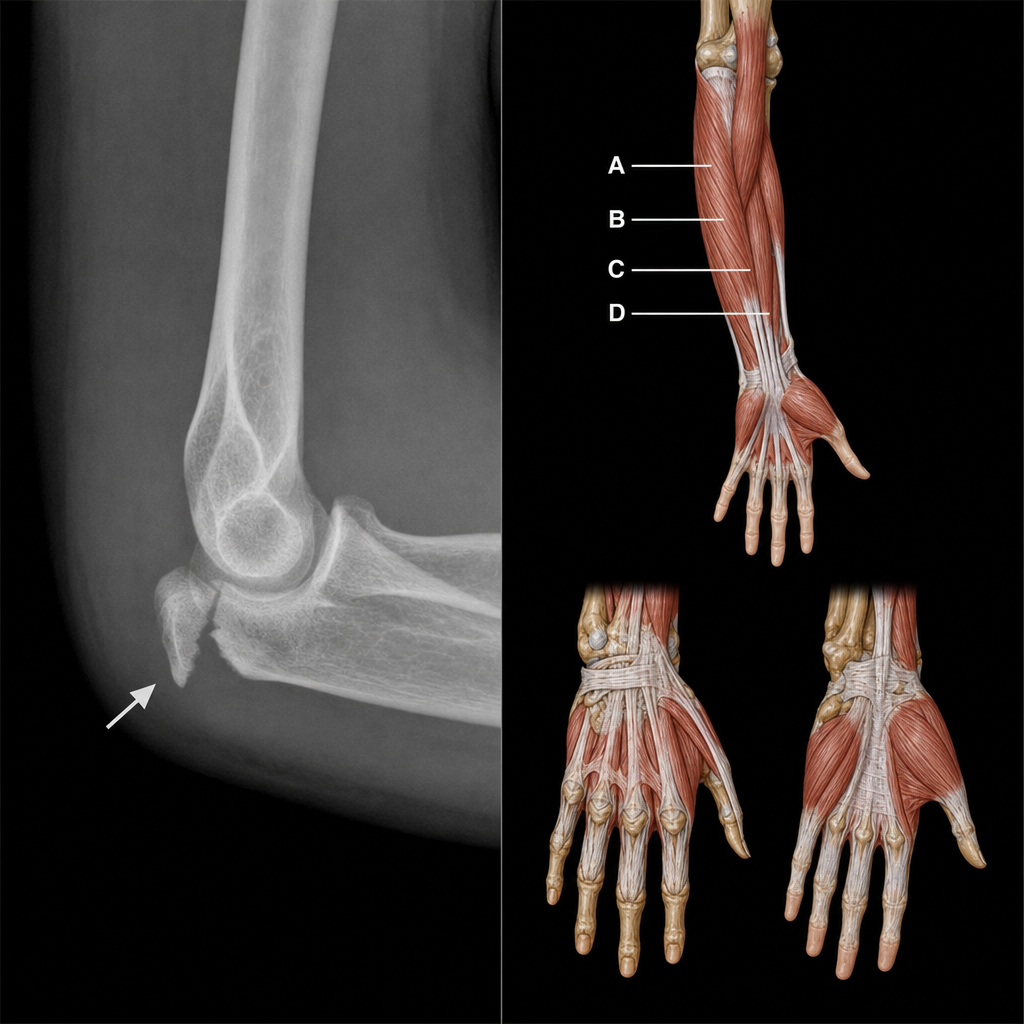
A 40-year-old male presented to the emergency room after a minor motorcycle accident, complaining of right elbow pain. An X-ray revealed a fracture of the medial epicondyle, and physical examination showed loss of sensation over the medial one and a half fingers and weakness of intrinsic hand muscles. The image below labels four intrinsic muscles of the hand (A–D). Which of the following muscles of the hand would be spared in this condition?
The upper lateral cutaneous nerve of the arm is a branch of which nerve?
Saturday night palsy affects which nerve?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app