
Upper Limb — MCQs

On this page
Which structure lies superficial to the bicipital aponeurosis in the cubital fossa?
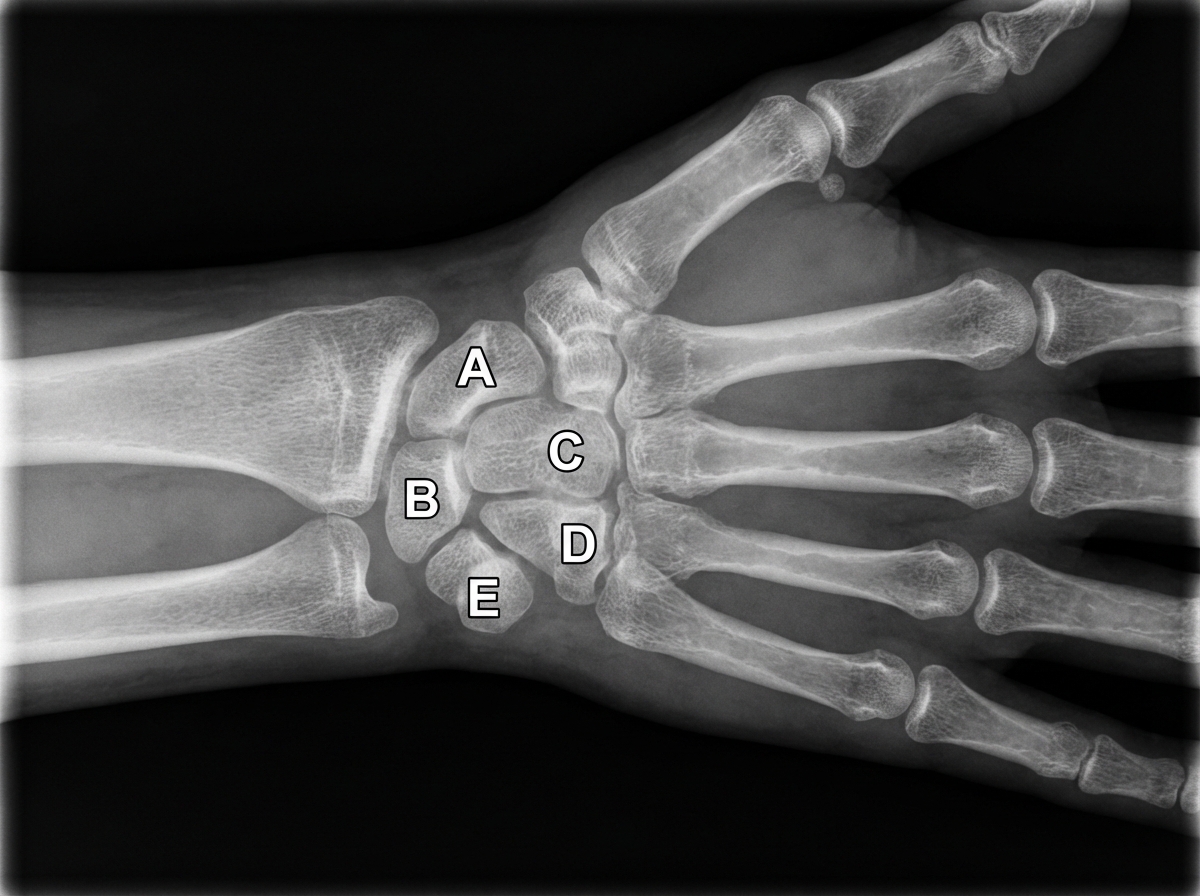
Destruction of the structure indicated by the letter E in the radiograph of the wrist and hand most likely causes weakness of which of the following muscles?
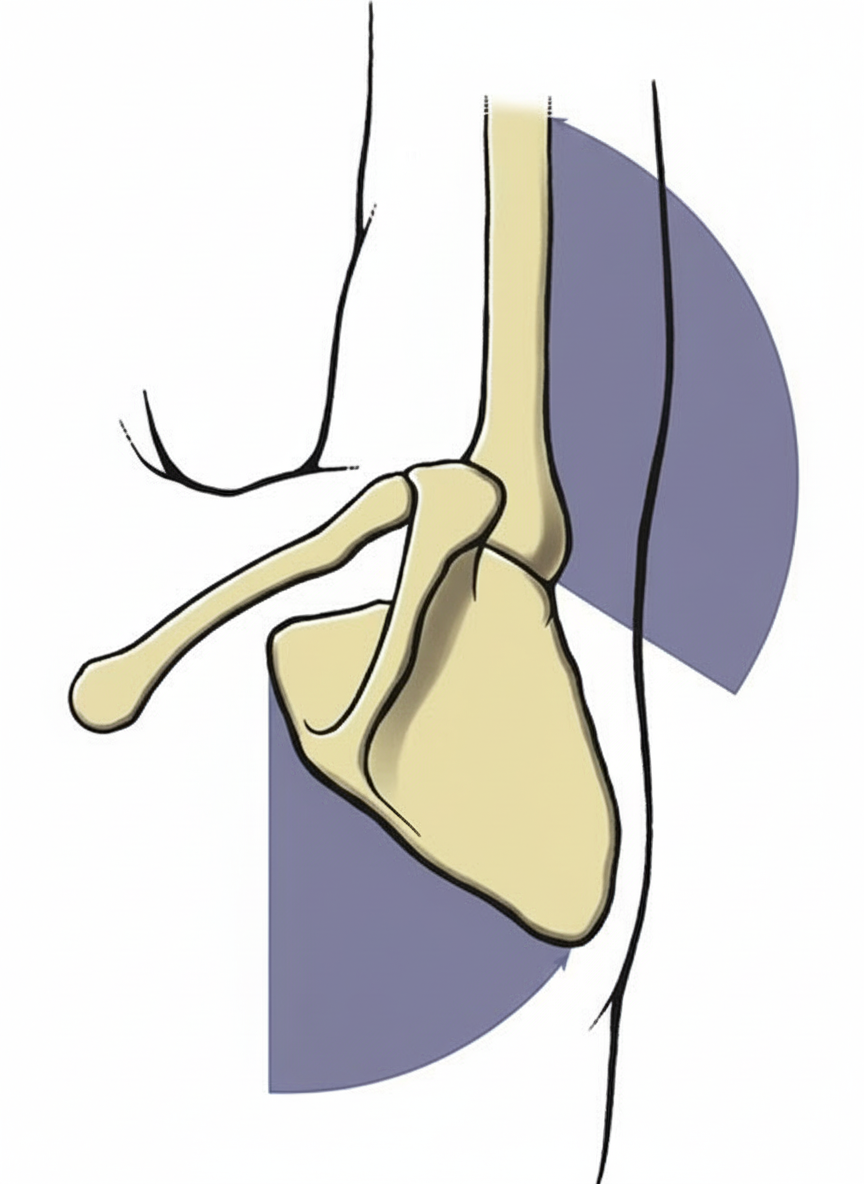
Which bone attaches the sternum to the scapula?
What is the most commonly used vein for intravenous injection?
A 52-year-old band director suffered problems in her right arm several days after strenuous field exercises for a major athletic tournament. Examination in the orthopedic clinic reveals wrist drop and weakness of grasp but normal extension of the elbow joint. There is no loss of sensation in the affected limb. Which nerve was most likely affected?
All of the following are true regarding the axillary artery except?
What are the root values of the nerves supplying the muscles needed for the latter part of the following action?
Apposition of the thumb involves which of the following movements?
Finger drop with no sensory loss is an injury of which nerve?
All of the following are muscles of the rotator cuff except?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app