
Upper Limb — MCQs

On this page
The lesion of Klumpke's paralysis is in which part of the nerve plexus?
A 42-year-old female presents with a shoulder injury requiring surgical repair of the supraspinatus muscle. Which of the following is true of the supraspinatus muscle?
A 40-year-old man sustains a left elbow fracture in a car accident. He presents with numbness in his fourth and fifth fingers, and a weakened hand grip. Neurologic examination reveals diminished sensation over the fifth finger and the ulnar aspect of the fourth finger, along with weakness in finger abduction and adduction. What is the most likely diagnosis?
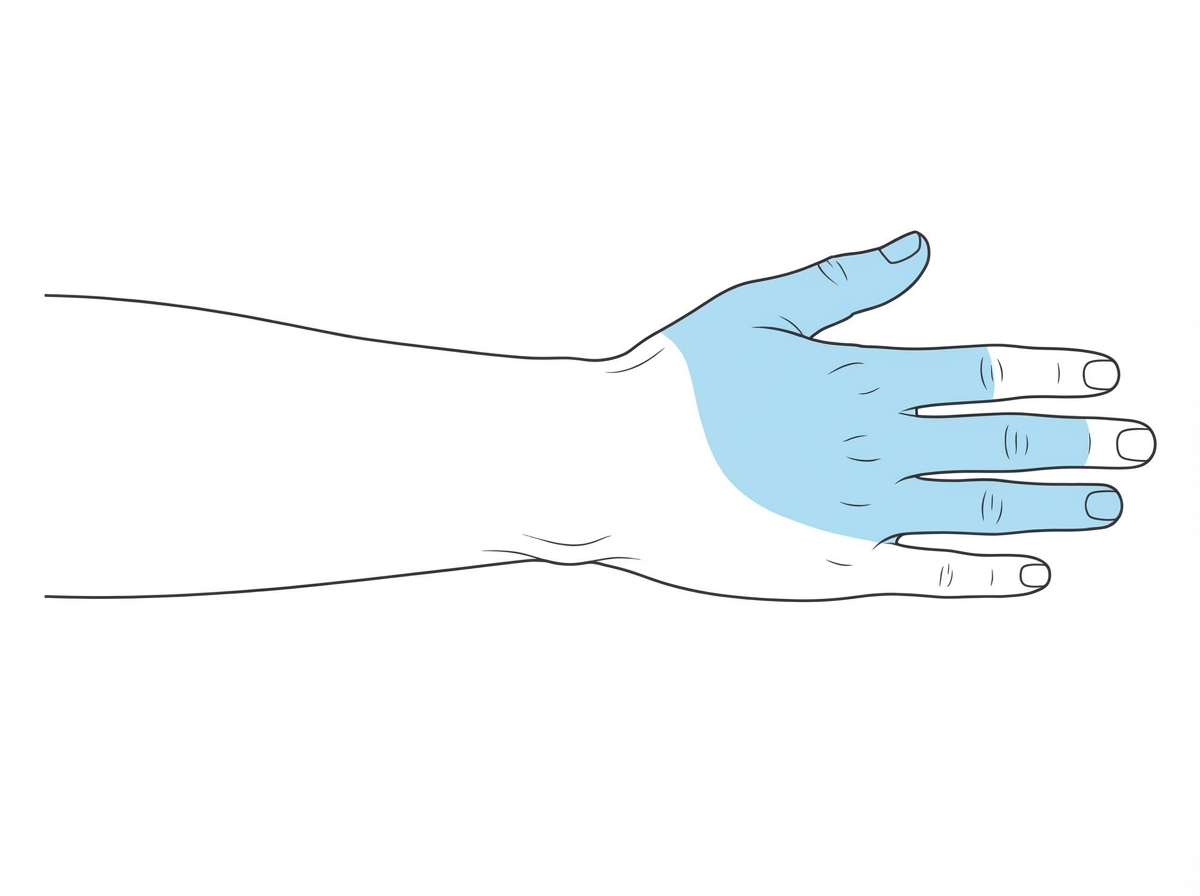
What is the sensory supply to the specified region?
A patient presents with hypothenar muscle wasting and loss of sensation of the medial one and a half digits. Which nerve is involved?
All the following are true regarding the Brachial plexus EXCEPT?
What is the largest bursa in the body?
Abduction and lateral rotation of the shoulder are primarily caused by nerve roots originating from which spinal segments?
Which of the following statements about Erb's palsy is TRUE?
Where is the insertion of the pectoralis major muscle located?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app