
Upper Limb — MCQs

On this page
A patient with leprosy presents with clumsiness of the hand due to ulnar nerve involvement. Palsy of which muscle group would cause this clumsiness?
Which of the following is false regarding Klumpke's paralysis?
Which cervical nerve root supplies the thumb dermatome?
A 50-year-old woman presented with numbness and weakness of the right hand. On examination, there was atrophy of the thenar eminence and hypoaesthesia in the distribution. Compression of which of the following nerves could explain the presentation?
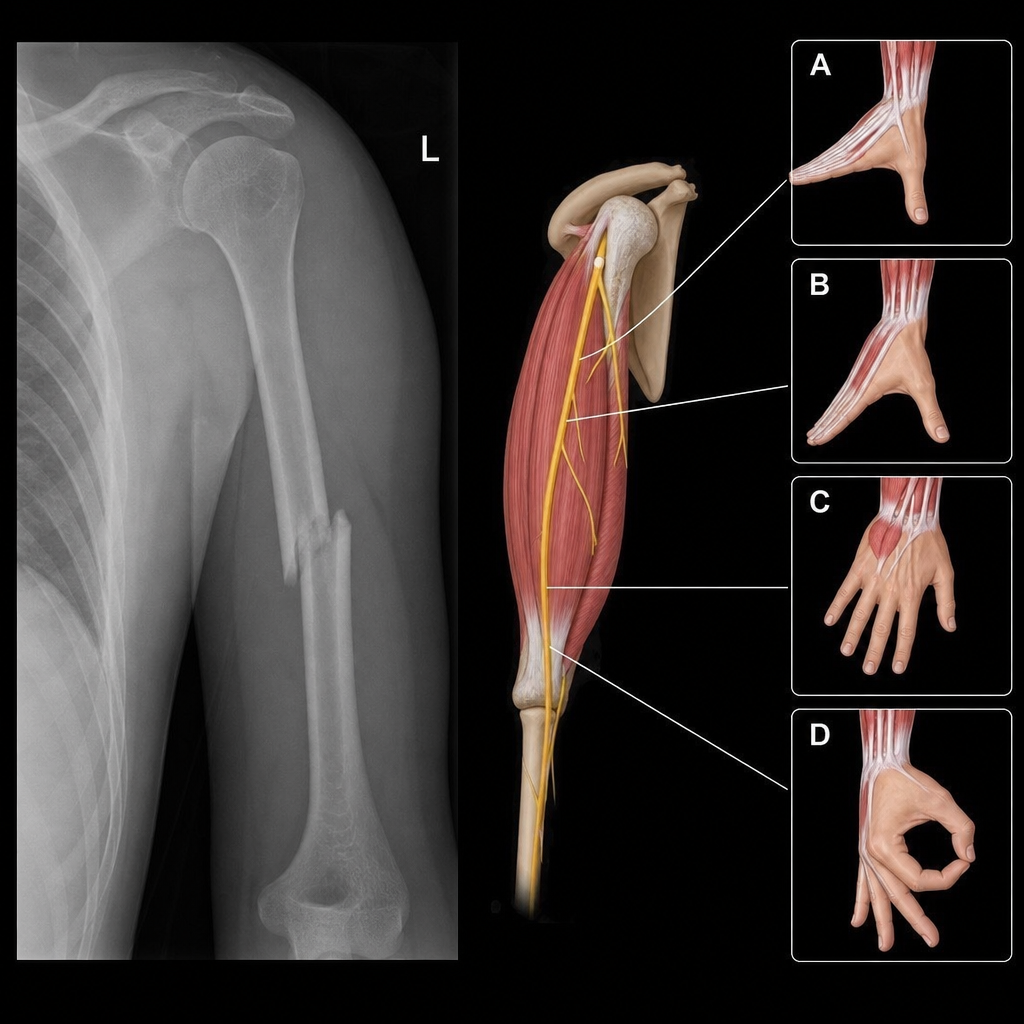
A 40-year-old male patient presented to the ER with pain and deformity in the left arm after a fall. An x-ray of the affected area was ordered. The nerve most likely involved in this condition supplies which of the following muscles?
Which arteries form the arterial anastomosis around the shoulder?
A man is unable to hold typing paper between his index and middle fingers. Which of the following nerves was likely injured?
Which of the following clinical signs is observed in median nerve injury?
The axillary artery is divided into three parts by which muscle?
A 32-year-old man presents with multiple fractures of his right upper limb following a severe car crash. He underwent surgery with fixation of bony fragments using metallic plates. Five months postoperatively, he presents with the ability to abduct his arm and extend his forearm. Sensation in the forearm and hand is intact. However, his hand grasp is very weak, and he cannot extend his wrist against gravity. Which of the following nerves was most likely injured during the surgical procedure?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app