
Upper Limb — MCQs

On this page
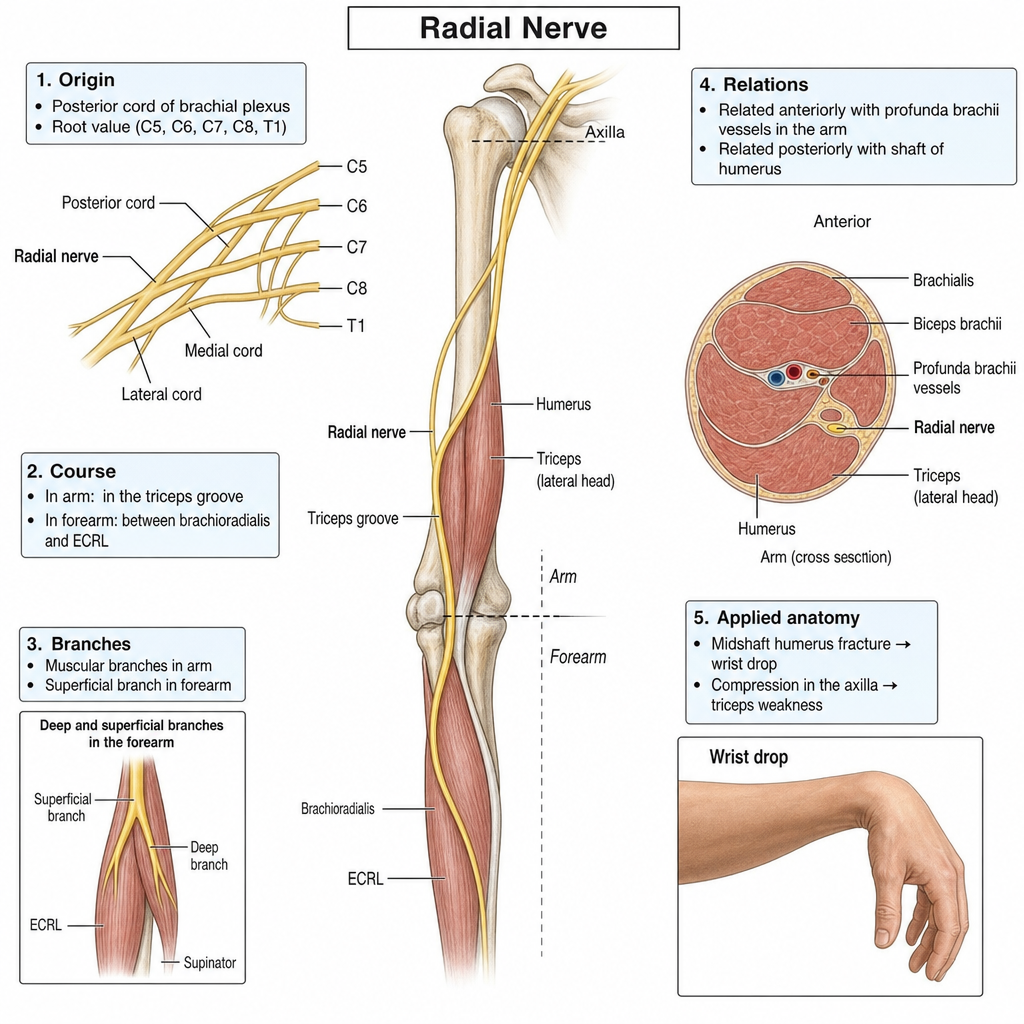
A 7-year-old boy falls from a tree house and is brought to the emergency department. On examination, he has weakness in rotating his arm laterally due to a nerve injury. Which of the following conditions is most likely to cause a loss of this nerve function?
Which of the following statements about the radial nerve are true? 1. It arises from the posterior cord of the brachial plexus. 2. It enters the arm behind the brachial artery and passes through the lower triangular space (with the profunda brachii artery) to reach the spiral groove. 3. It supplies all three heads of the triceps brachii and the anconeus before entering the forearm. 4. It supplies the skin over the medial side of the arm. 5. Injury in the spiral groove (e.g., humerus fracture) leads to wrist drop due to paralysis of the extensors of the wrist and digits.
Which of the following statements regarding the deep palmar arch is TRUE?
Which of the following statements is false regarding the radial nerve?
The coracoid process is what type of epiphysis?
Injury to the C7 nerve root will result in loss of sensation in which area of the arm?
Atrophy of intrinsic muscles of the hand, sensory deficit on the medial side of the forearm and hand, and diminished radial pulse on turning the head to the affected side could be due to which of the following conditions?
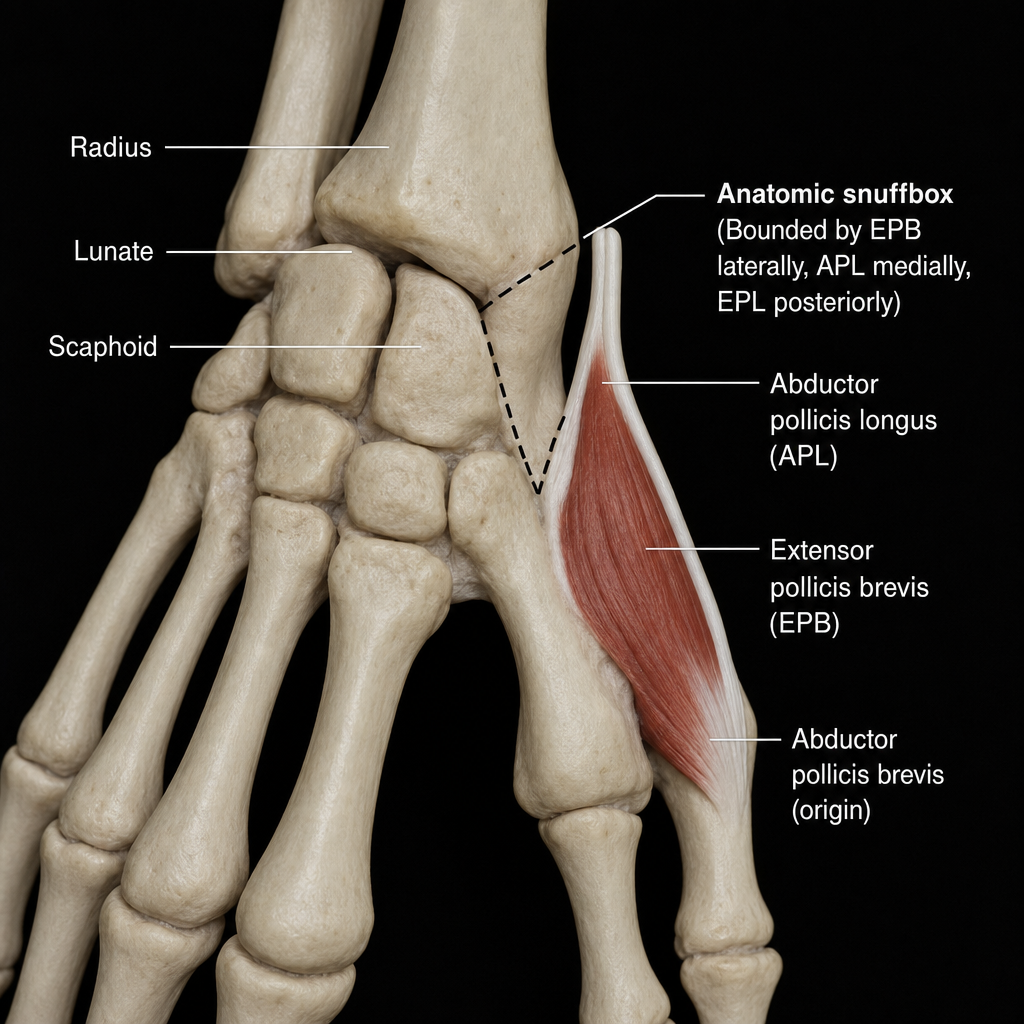
If the floor of the anatomic snuffbox and origin of the abductor pollicis brevis are damaged, which of the following bones in the proximal carpal row is most likely to be involved?
A 12-year-old patient presents with a severely damaged nail on their index finger after accidentally crushing the finger while closing a door. A decision is made to excise the injured nail. In preparation for the procedure, the physician would most likely anesthetize a branch of which of the following nerves?
Wrist drop is due to injury to which nerve?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app