
Upper Limb — MCQs

On this page
A 45-year-old woman presents with neck pain. An MRI reveals a herniated disk in the cervical region. Physical examination demonstrates weakness in wrist extension and paresthesia on the back of her arm and forearm. Which of the following spinal nerves is most likely injured?
The capitate bone articulates with all of the following EXCEPT:
Compression of a nerve within the carpal tunnel produces inability to?
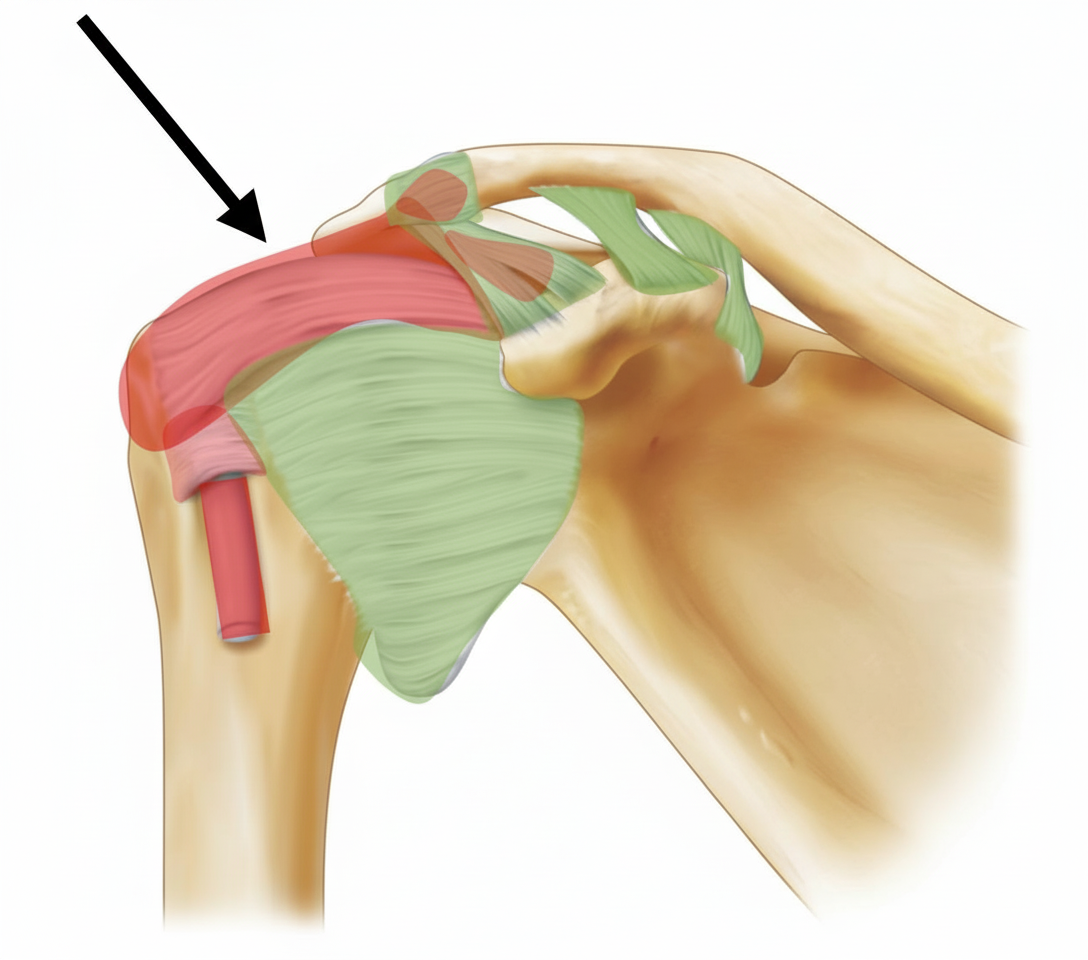
Identify the ligament:
Which of the following statements best describes the pectoral girdle and shoulder?
Which tendon is absent in the palm?
A 69-year-old man has numbness in the middle three digits of his right hand and finds it difficult to grasp objects with that hand. He has atrophy of the thenar eminence. Which of the following conditions is the most likely cause of the problems in his hand?
Ulnar paradox is seen in which of the following conditions?
All of the following structures pass through the deltopectoral triangle, EXCEPT?
A patient loses the ability to flex their forefinger. The nerve that supplies the muscles responsible for this action is formed from which of the following cord(s) of the brachial plexus?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app