
Upper Limb — MCQs

On this page
Which artery passes through the upper triangular space?
What is the nerve supply of the rhomboid major muscle?
Main-Gruber connections are:
Which muscle is supplied by the dorsal scapular nerve?
What is the most appropriate ending for the sentence: The median nerve:
Which muscle is spared in Erb's palsy?
A 17-year-old boy with a stab wound received multiple injuries on the upper part of the arm and required surgery. If the brachial artery were ligated at its origin, which of the following arteries would supply blood to the profunda brachii artery?
What type of joint is the wrist joint?
Median nerve injury at the wrist causes what functional deficit?
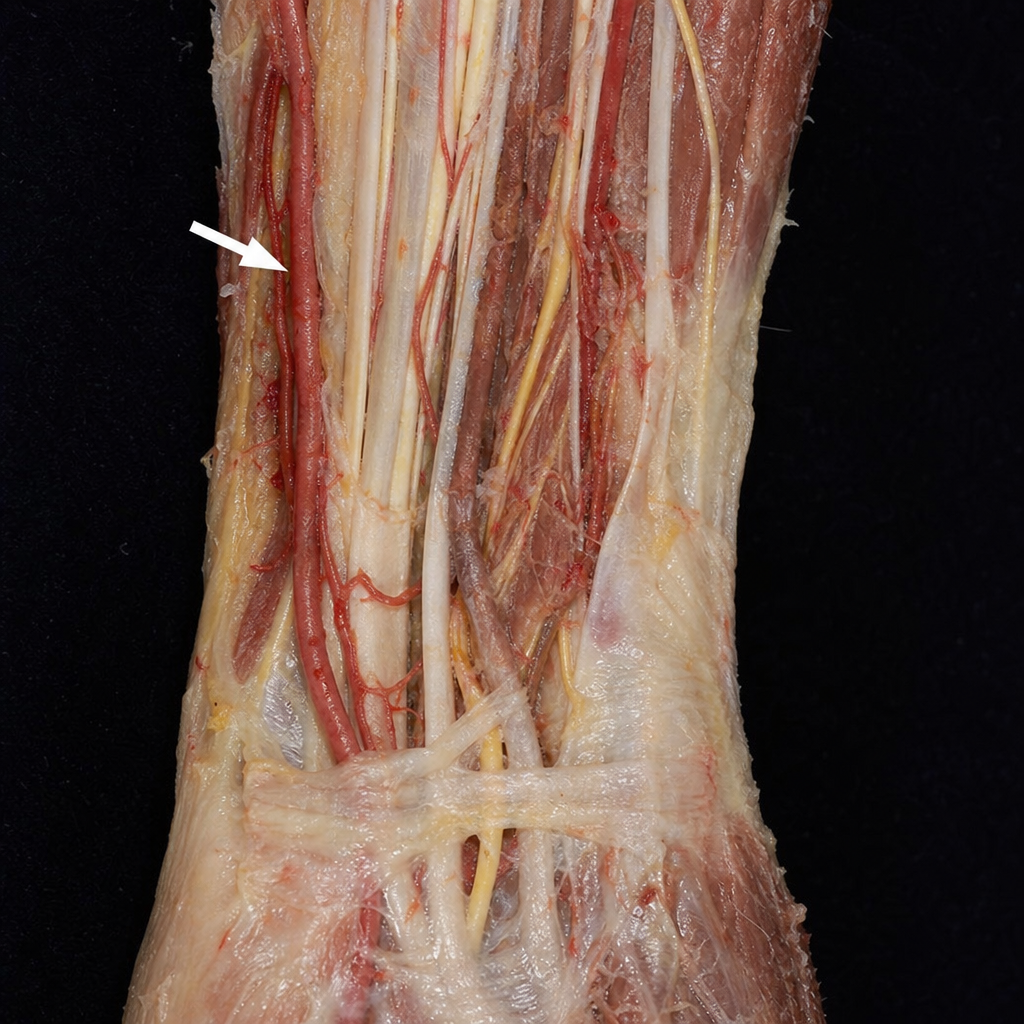
Which structure is present in the area marked by the arrow?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app