
Upper Limb — MCQs

On this page
A 29-year-old patient has a dislocated elbow in which the ulna and medial part of the distal humerus have become separated. What classification of joint is normally formed between these two bones?
A 26-year-old male sustained a mid-arm injury, resulting in wrist drop, finger drop, loss of sensation on the dorsum of the hand, but with preserved elbow extension. What is the most likely diagnosis?
Which of the following bones has its head located at the epiphysis?
Which nerve is not related to the humerus?
Which muscle has dual nerve supply?
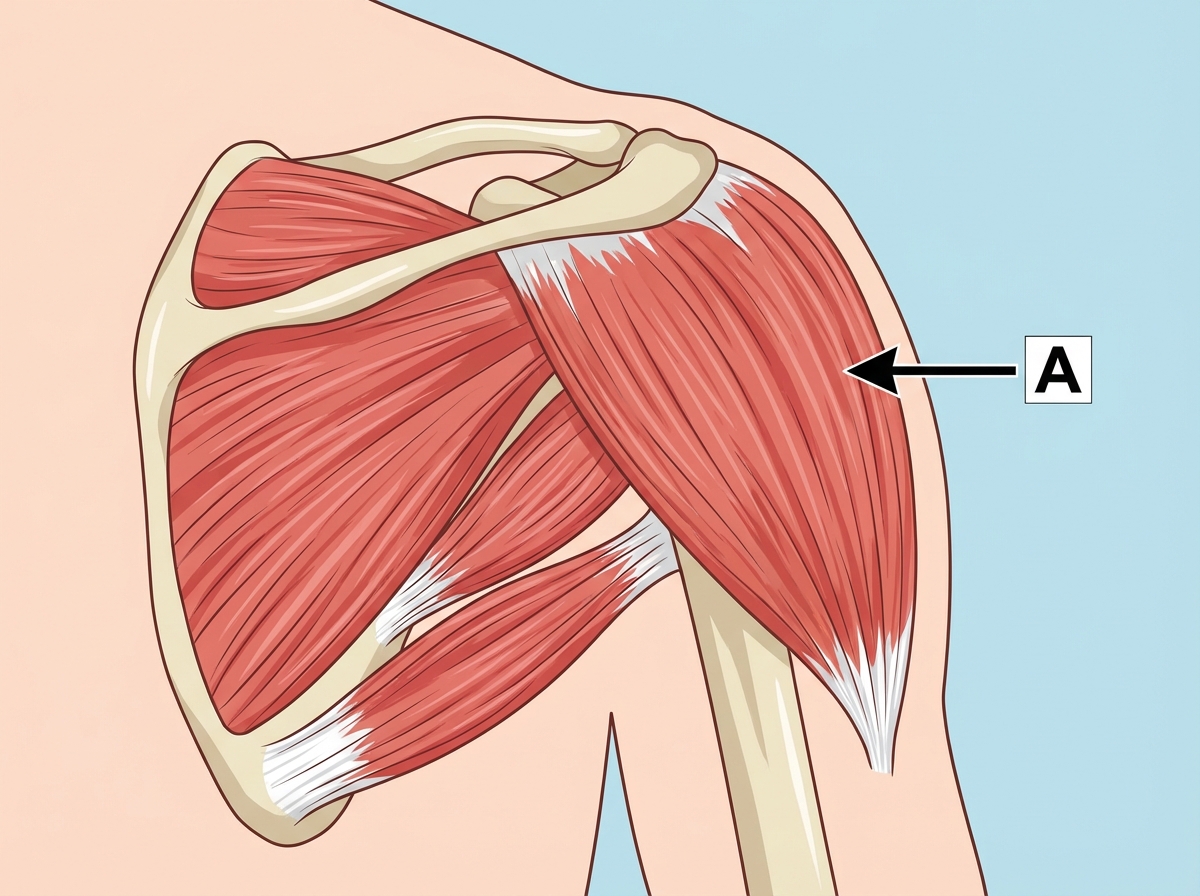
Which nerve supplies the muscle marked A?
All the thenar muscles of the hand are supplied by the median nerve except?
Which spinal nerve roots primarily supply the intrinsic muscles of the hand?
A 35-year-old man presents with a stab wound to the most medial aspect of the proximal portion of the cubital fossa. Which of the following structures would most likely be damaged?
A boy presents with injury to the medial epicondyle of the humerus. Which of the following would not be seen?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app