
Upper Limb — MCQs

On this page
Identify the muscle along with its action.
Match the corresponding structures according to the labels in the given image.
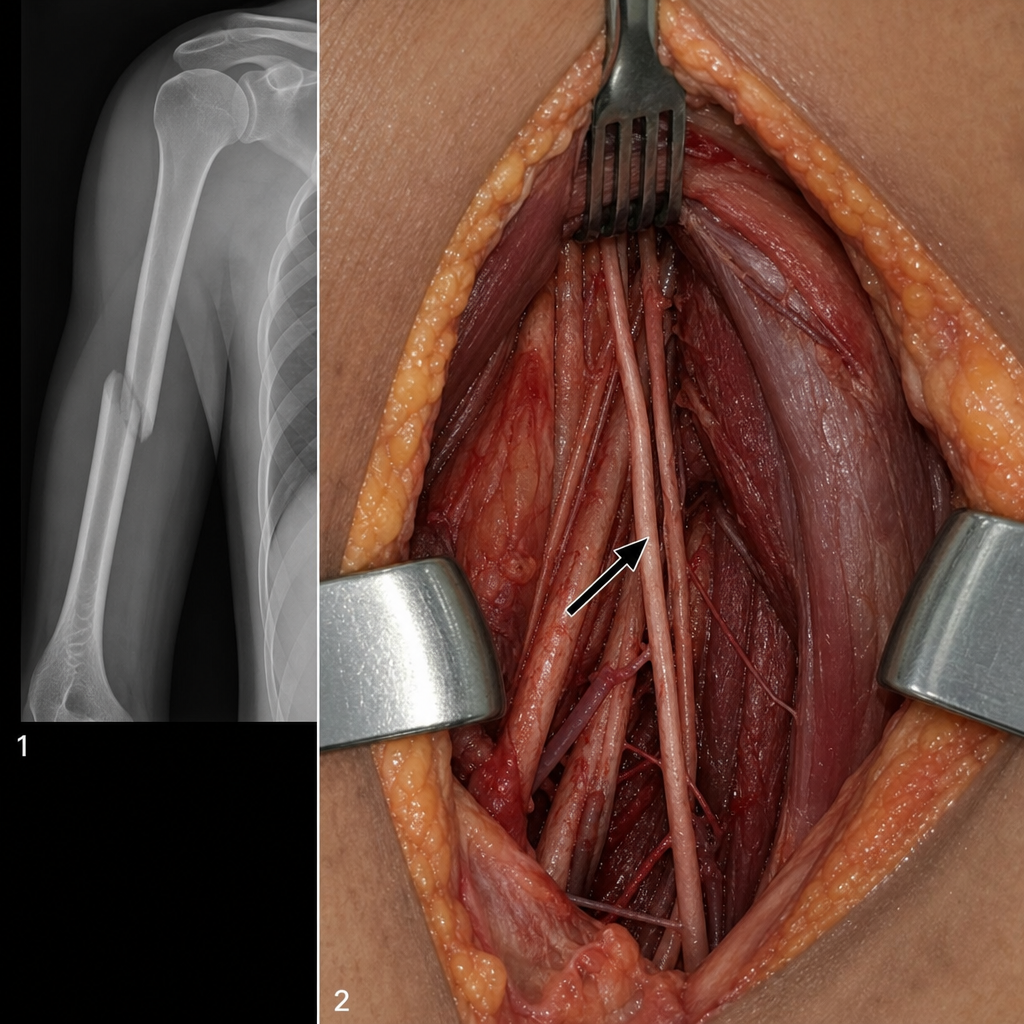
A person came in with difficulty to abduct his left arm above 15 degrees and loss of sensation over his left lateral arm. Xray of the affected arm is given. Which structure is most probably affected? (Badge sign was also mentioned in the question).
A 34-year-old man sustains a mid-shaft fracture of the humerus following a road traffic accident. During the axillary surgical approach for fixation, the operating surgeon identifies and tags a nerve (arrowed in Image 2) based on its intraoperative course and relationships — not solely on the fracture pattern. Postoperatively, the patient has weakness of elbow flexion and loss of sensation over the lateral forearm, consistent with injury to the tagged nerve. The nerve was identified intraoperatively as it pierced a muscle of the anterior axillary wall, and the image shows this tagged nerve with a clear arrow at the point of entry. Which statement best describes the course of the tagged nerve that accounts for both the motor and sensory deficits seen in this patient?
What is true about the blood supply of the scaphoid bone?
Practice by Chapter
Pectoral Region and Axilla
Practice Questions
Arm and Cubital Fossa
Practice Questions
Forearm and Hand
Practice Questions
Joints of Upper Limb
Practice Questions
Nerves of Upper Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy and Landmarks
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app