
Surface and Radiological Anatomy — MCQs

On this page
To what level of vertebrae does the marked structure correspond?
On palpation at the site marked by the red arrow on the image, a bony ridge is felt. What is the vertebral level of the marked arrow?
Identify the rib highlighted in the X-ray.
In the given barium swallow image, which of the following shows the left atrium impression on the esophagus?
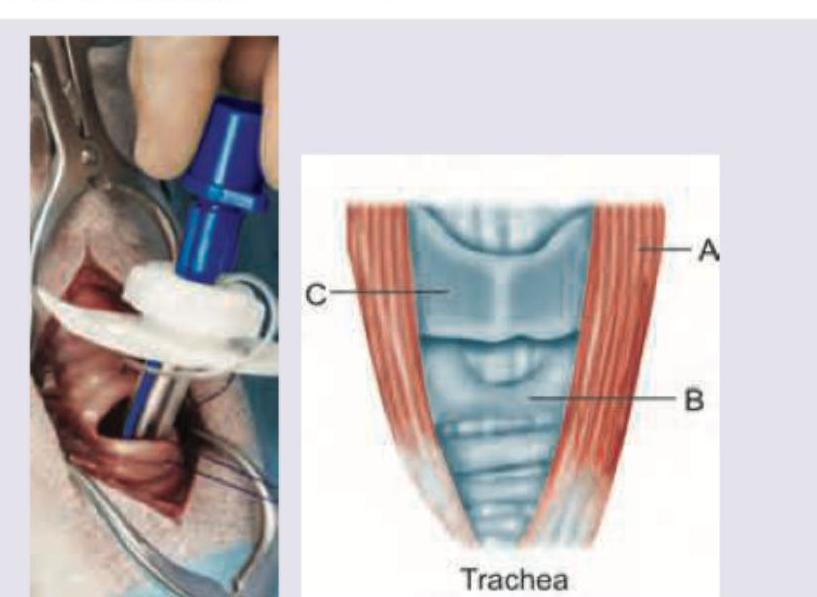
The following procedure is being performed. Identify the markings:
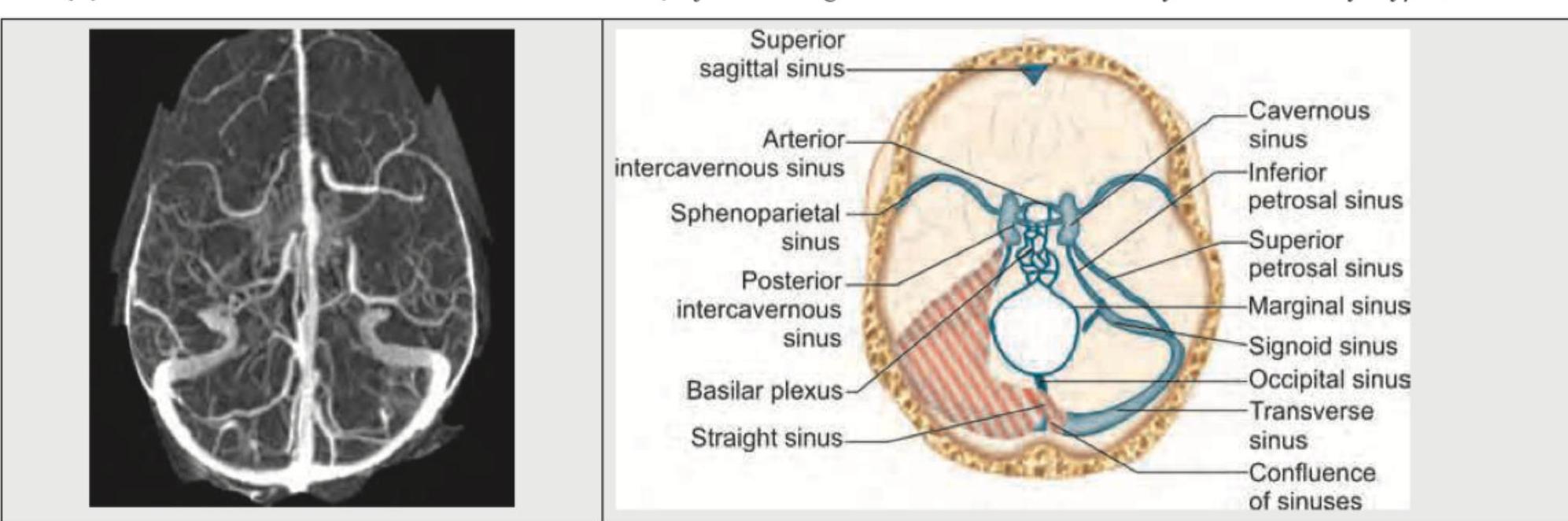
Identify the anatomical structure shown in the image.
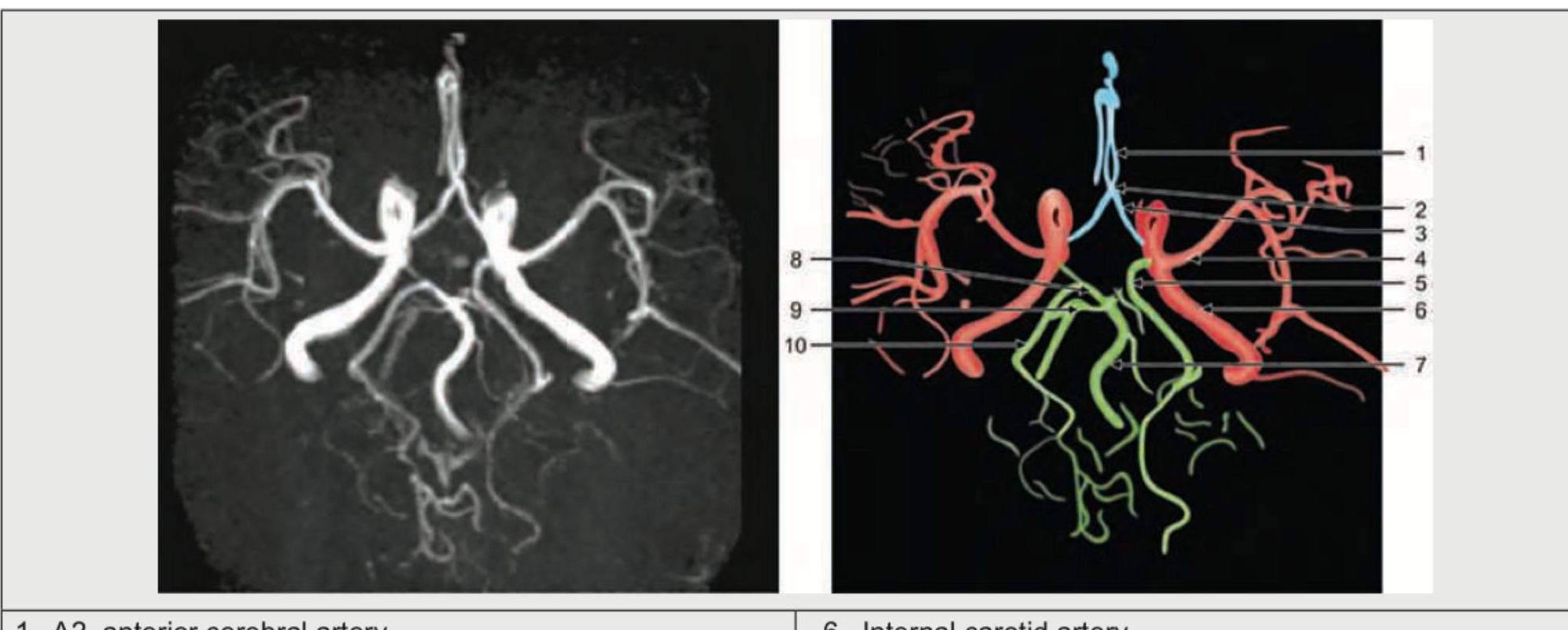
Identify the marked blood vessel in the image.
The structure shown below is:

Name the structure marked as $X$ in the CT abdomen shown below: (Recent NEET Pattern 2016-17)

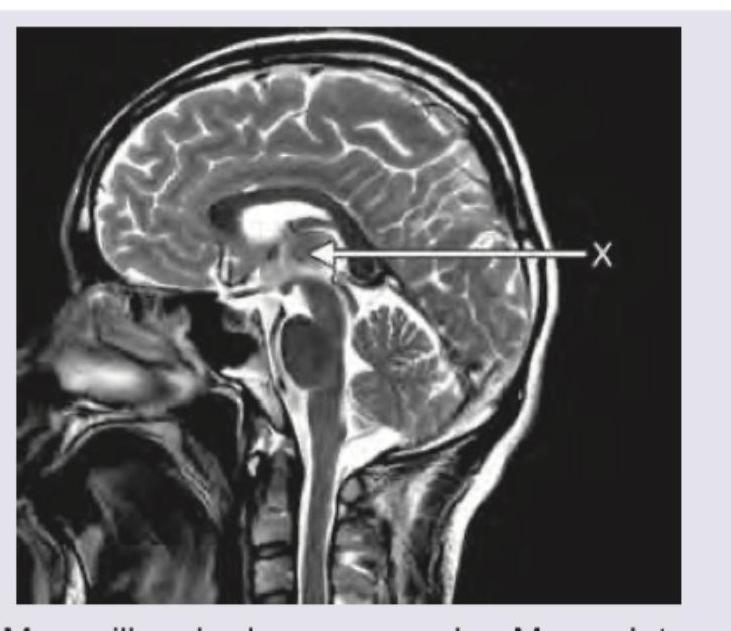
The area marked in MRI is:
Practice by Chapter
Surface Landmarks of the Head and Neck
Practice Questions
Surface Landmarks of the Thorax
Practice Questions
Surface Landmarks of the Abdomen
Practice Questions
Surface Landmarks of the Limbs
Practice Questions
Radiographic Anatomy
Practice Questions
CT Anatomy
Practice Questions
MRI Anatomy
Practice Questions
Ultrasonographic Anatomy
Practice Questions
Angiographic Anatomy
Practice Questions
Sectional and Cross-sectional Anatomy
Practice Questions
Anatomical Correlations in Common Imaging
Practice Questions
Interventional Radiological Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app