
Surface and Radiological Anatomy — MCQs

On this page
The aortic component of the second heart sound is best heard at which anatomical location?
What is the surface marking of the arch of the aorta?
Which spinal segment supplies the umbilicus?
McBurney's point is located at which position on the abdomen?
Which of the following structures is NOT found at the transpyloric plane?
The common carotid artery is palpable at which anatomical landmark?
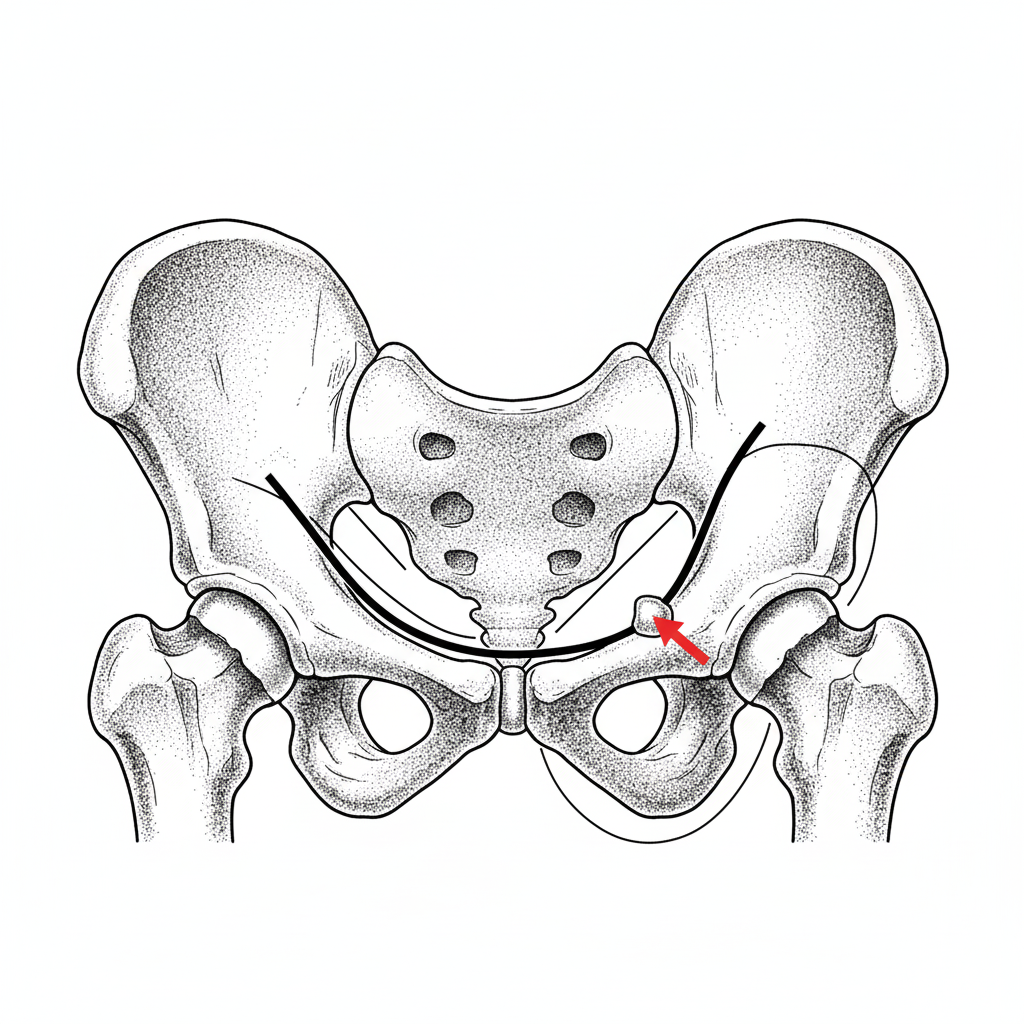
Shenton's line is:
The bony landmark shown in the diagram is used to differentiate between inguinal and femoral hernias. What is this landmark?
The P2 heart sound is best appreciated in which location?
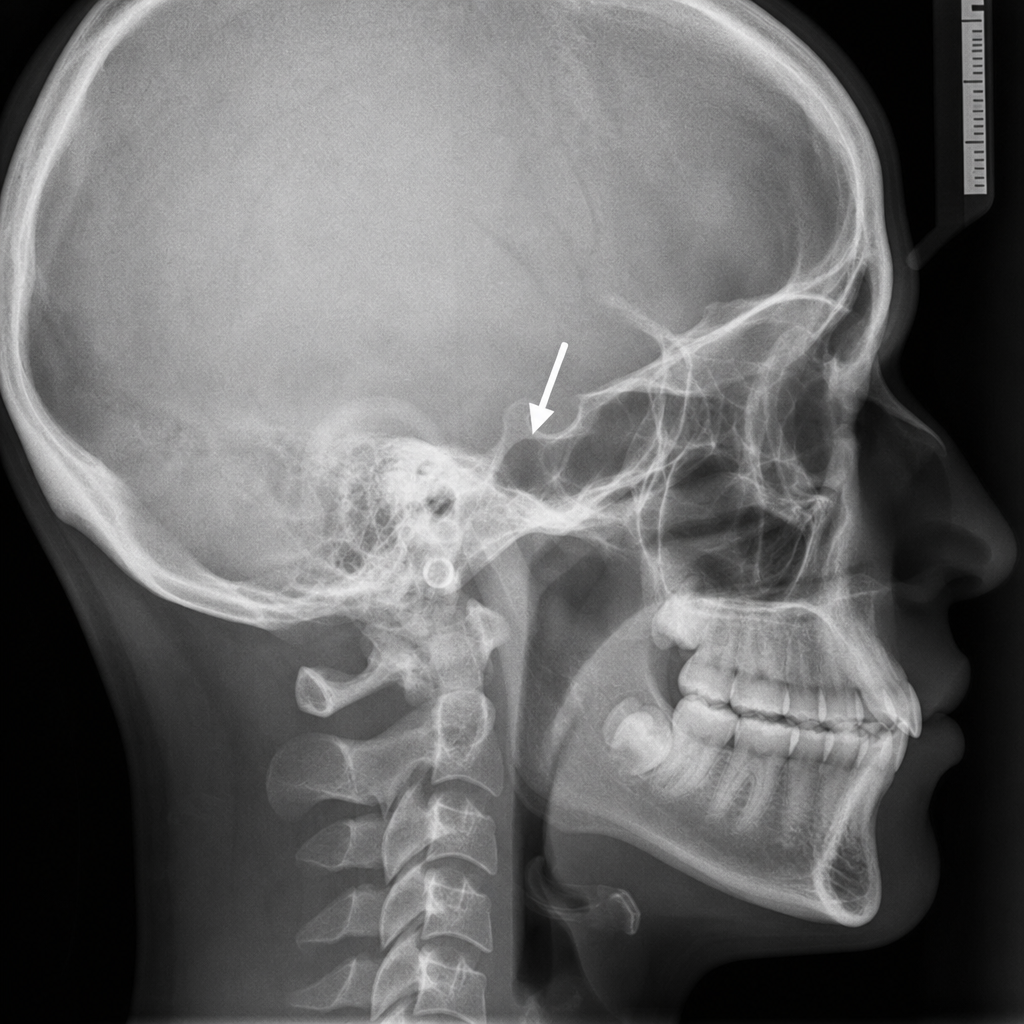
The marked structure on the X-ray is:
Practice by Chapter
Surface Landmarks of the Head and Neck
Practice Questions
Surface Landmarks of the Thorax
Practice Questions
Surface Landmarks of the Abdomen
Practice Questions
Surface Landmarks of the Limbs
Practice Questions
Radiographic Anatomy
Practice Questions
CT Anatomy
Practice Questions
MRI Anatomy
Practice Questions
Ultrasonographic Anatomy
Practice Questions
Angiographic Anatomy
Practice Questions
Sectional and Cross-sectional Anatomy
Practice Questions
Anatomical Correlations in Common Imaging
Practice Questions
Interventional Radiological Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app