
Surface and Radiological Anatomy — MCQs

On this page
Surface marking of the internal jugular vein is obtained by joining which two points?
Which of the following does NOT form the right heart border?
What is the approximate distance of the gastroesophageal junction from the upper incisors?
What is the area for auscultation overlying the chest wall that is best suited for the aortic area?
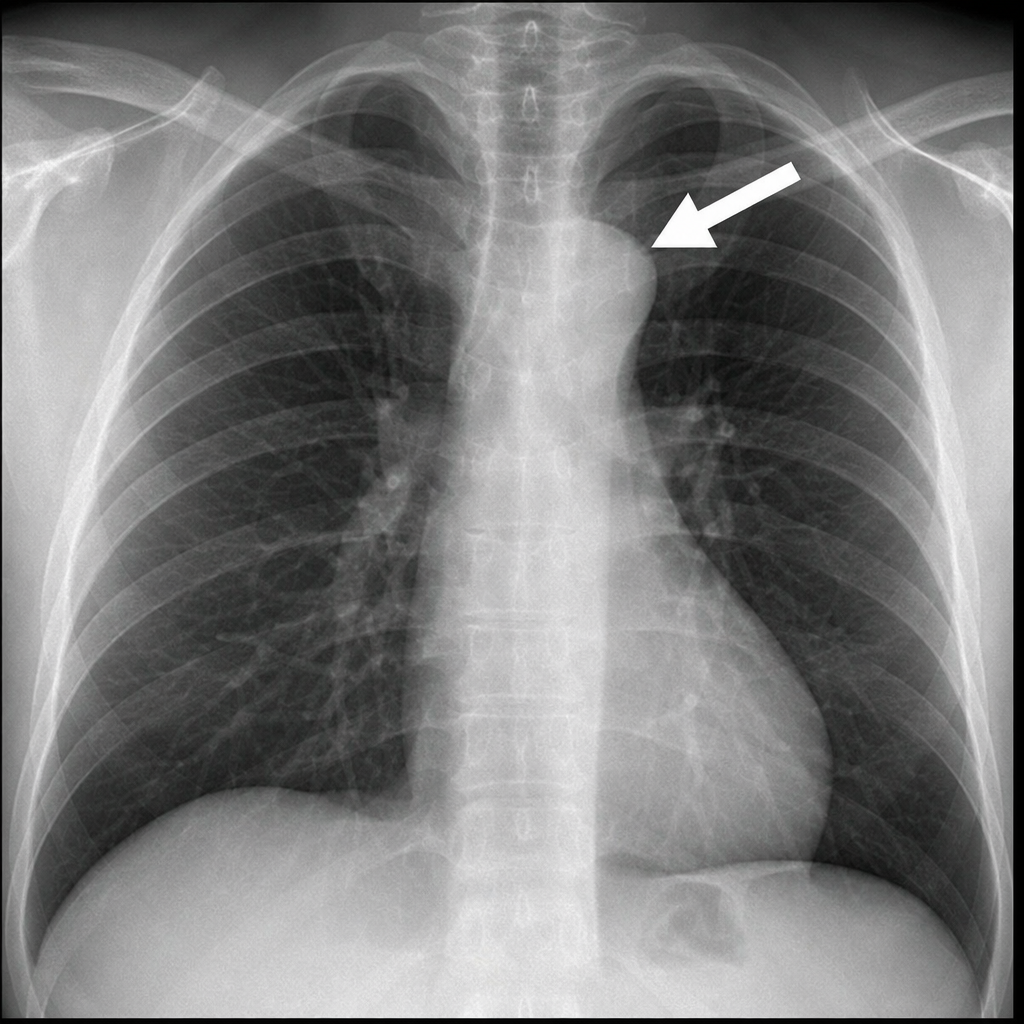
A 41-year-old male presents with shortness of breath, dizziness, and sharp chest pain. The large arrow in his chest radiograph indicates the region of pathology. What is this structure?
Which of the following represents the surface marking of the aortic valve?
Which of the following structures does not form the right border of the heart on an X-ray?
The inferior angle of the scapula is typically located at which vertebral level?
Which of the following does not contribute to the hilar shadow?
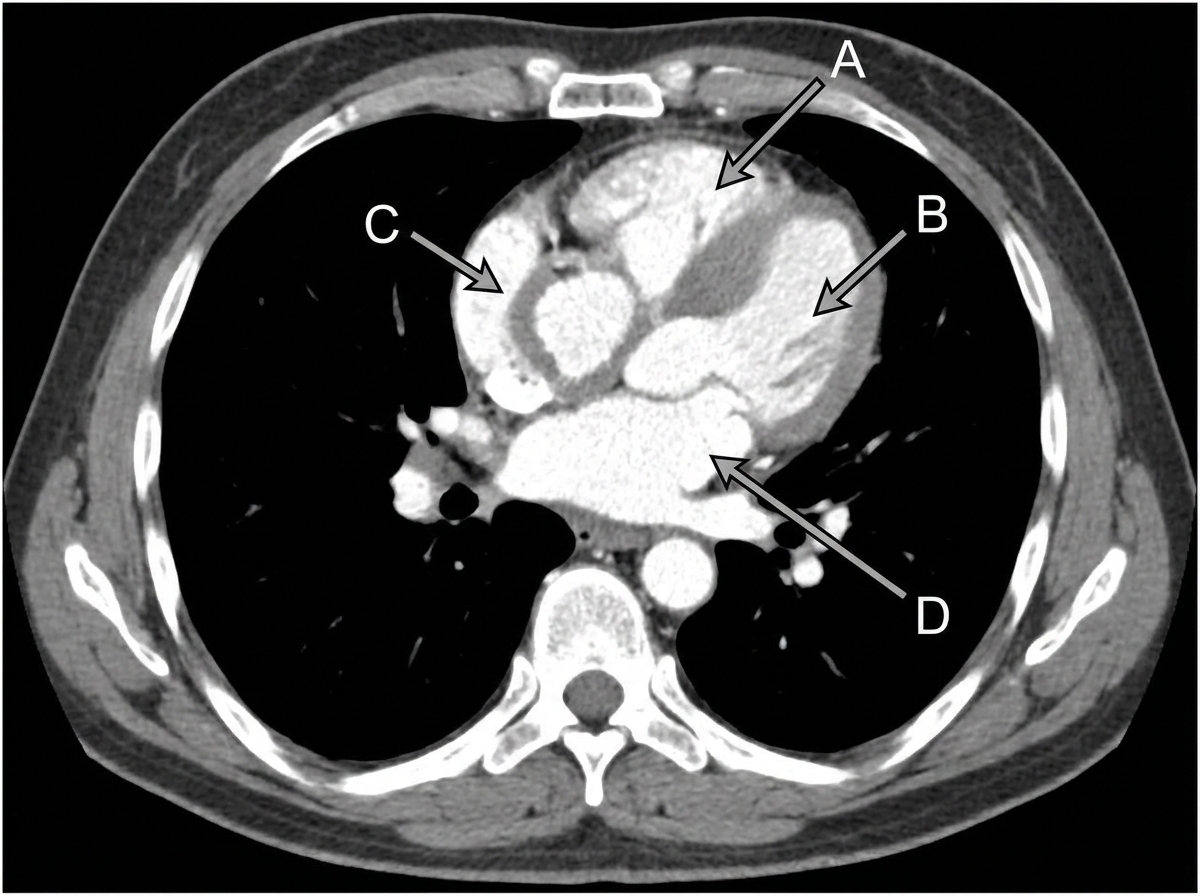
In a CT scan of the thorax, which labeled site or structure becomes hypertrophied as a result of pulmonary stenosis?
Practice by Chapter
Surface Landmarks of the Head and Neck
Practice Questions
Surface Landmarks of the Thorax
Practice Questions
Surface Landmarks of the Abdomen
Practice Questions
Surface Landmarks of the Limbs
Practice Questions
Radiographic Anatomy
Practice Questions
CT Anatomy
Practice Questions
MRI Anatomy
Practice Questions
Ultrasonographic Anatomy
Practice Questions
Angiographic Anatomy
Practice Questions
Sectional and Cross-sectional Anatomy
Practice Questions
Anatomical Correlations in Common Imaging
Practice Questions
Interventional Radiological Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app